



Death, Taxes and… Presbyopia?
So here I am, comfortably into my 40s. In many ways, this is a grand time of life: satisfying career, happy home, a greater sense of well-being and contentment. But over the last couple of years, spectacles sit on the bridge of my nose more often than not, for any close-up activity. It started in my 30s: +1 “readers” when I was using the computer a lot. Not a big deal. And the tortoise shell frames looked cute, I thought. But then, seemingly overnight, the +1s became +1.5s; and shortly thereafter, +2.0s. Recently, when I was gunning for a pair of +2.5s, I said,“Enough!” I expressed my dismay to an ophthalmologist friend; he laughed and said, “Welcome to middle age!”
Death and taxes. Maybe. But presbyopia? Noooooo! Isn’t there something that functional medicine can offer which will curtail this rather irritating but inevitable rite of passage?
First of all, what IS presbyopia?
100% of us experience it between 40 and 50 years of age. That’s right, 100%. This means that more than a billion of us are presbyopic right now. (By comparison, the epidemic of diabetes claims about 350 million.) The change actually starts happening at about 20 years of age — but we don’t notice it.

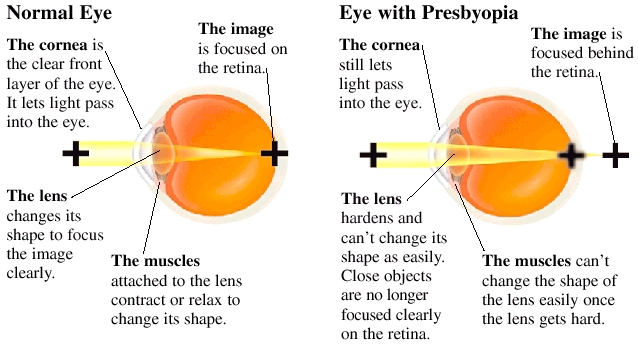
Figure 1: Basic anatomy of the eye.

Figure 2: The very basics of presbyopia
{kind=link}
A few main processes seem to be occurring that underlie presbyopia. Understanding these gives us insight into a possible functional approach to treatment. One, the lens becomes sclerotic (hardened); and lens transparency (which is near-perfect in youth) is progressively lessened. This means that both seeing AND focusing on close objects (accommodation) becomes more difficult. The lens also continues to grow throughout life (about 20 µm per year), which means that the distance between the lens and the ciliary muscles (part of the ciliary body; see figure 1) is shortened. The ciliary muscles respond to this reduced distance by shortening themselves. The end result is that the force the ciliary muscles can apply to the lens is lessened, resulting in decreased ability to accommodate, or focus, on objects close up. Make sense? Think of it like tight hamstrings and reduced ability to fully extend your legs (only your legs don’t keep growing throughout life).
If you’re a functional medicine clinician, no doubt you’re wondering right now what causes the lens rigidity and loss of transparency. You’ve probably got a few ideas. Increased oxidative stress? Certain environmental factors? Yes to both.
Indeed, our ability to transport the all-important glutathione to the lens nucleus declines with age. Oxidized glutathione and dehydroascorbate (oxidized vitamin C) accumulate as we age. And we are less able to clear out the denatured/oxidized lens proteins via the ubiquitin-proteasome pathway as we get older. Furthermore, the accumulation of damaging advanced glycation end products (AGEs) — sugars binding to lens proteins — leads to loss of lens transparency. This is akin to the elevation of hemoglobin A1C that we see in diabetics.
Concurrently, the lenses are exposed to more oxidizing (hence damaging) environmental agents over the course of aging: UVA, cigarette smoke, chemicals (such as hair dyes) — all have been shown to damage the lens and contribute to presbyopia. This is of course compounded by our reduced ability to respond to the oxidative assault.
Incidentally, these same underlying biochemical lesions — left unchecked — can form the basis of certain types of cataracts and macular degeneration.
Armed with this information, the start of a good treatment approach becomes clear. Note that these nutrients have shown benefit for cataracts and macular degeneration, not presbyopia. I am extrapolating that they should be at least somewhat useful for presbyopia, given the shared biochemical changes of each condition:
- Glutathione taken both orally and as eye drops (available through a compounding pharmacy, can obtain with carnosine)
- Vitamins C, E and A
- Zinc
- Classic antioxidant bioflavonoids: billberry, lutein, zeathanthin
- Carnosine eye drops have been shown to inhibit glycation (AGEs) and is used quite effectively for cataracts
- EPA/DHA
- Essential: Low glycemic diet (my preference is a Paleo-type diet)
But I’d be remiss to stop here. In fact, I’ve followed a modified version of the above without sufficient benefit; although I do think it’s important, make no mistake. We have to dig a little deeper. Regarding changes to the lens size and ciliary muscle length: surgical procedures are on the horizon and could be a realistic option at some point. This is akin to getting LASIX. We should also consider:
- “Screen-free time.” Computer workers-and anyone involved in close-up work- show a higher incidence of early onset presbyopia. (Smart phones fit here, too!)
- Eye exercises. Take the glasses off, move your eyes around in the cardinal directions.
- Don’t give into a stronger lens — or do so only for very close-up needs. Keep your eye muscles working.
- De-stress.
- Wear sunglasses- protect your eyes from UV radiation
- And finally, quite interesting work is happening in the area of adult neuroplasticity. That is, we can retrain our brains to see better. A particularly interesting study demonstrated that perceptual learning resulted in a complete correction of presbyopia in some and significant improvement in others.
- Conveniently, the lead author, Uri Polat, of the above study designed an app, Glasses Off, that when used three times per week for 12-15 minutes will result in significantly improved vision. Note that they used the program for 30 minutes three times per week in the study.
I will be trying a few of these ideas- evolving my current protocol of eye exercises, lower strength glasses and supplements. I’ll add in the glutathione/carnosine drops, and consider trying Glasses Off. I’ll keep you posted!

Bibliography
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3061107/pdf/rstb20100300.pdf
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3615154/pdf/aging-04-861.pdf