One Mushroom, Two Patients: A Practitioner’s Case for Targeted Lion’s Mane Formulation

My first EOE patient in the early 2000’s was fortunately, already diagnosed by a very savvy Yale gastroenterologist. I hadn’t heard of EOE at that time, but quickly learned about this highly challenging and potentially disabling mixed IgE allergic condition. It was clear immediately that functional medicine was the solution, and despite my lack of awareness of EOE, I had much to offer my first patient. Since then, we’ve seen more and more EOE patients in clinical practice, unfortunately, due to the meteoric rise of this condition. Fortunately, our tools continue to benefit.
Juston Jaco, a member of our nutrition team, outlines below his terrifying years-long journey with EOE, While we featured his powerful (and quite frankly, heartbreaking) story in our consumer blog, you’ll see that in the professional version below, Juston dives deeply into mechanisms (and solutions- see his handy reference table!). Thus, if you’ve already read his story, just skip down to the bolded “That is, until I started to do some research…” Thank you, Juston, for sharing your journey with us and your clear insights from synthesizing the literature on EOE. ~DrKF
*
I remember suffocating, unable to speak. I panicked and thought, quite hysterically, this is it.
I was 23 years old.
***
Truth be told, even though I convinced myself I was in good health, fear of asphyxiation surreptitiously lurked in the background of every meal I consumed from childhood. In fact, unlike most children, my memories at the dining room table were filled with worry and apprehension. I knew early on that I had to macerate each bite as if my life depended on it. If I didn’t completely pulverize my food, then I was setting myself up to choke to death.
The antagonism between me and the doctors who said “it’s all in your head” grew until I was formally diagnosed with eosinophilic esophagitis (EoE) at 18 in 2010. The liquid and inhaled corticosteroid prescription drugs did not work at assuaging my symptoms, rather my choking spells became more severe. I quite honestly felt one swallow away from death, and no one knew how to help. At the same time, I was battling seasonal allergies, bacterial acne, migraine headaches, hair loss, anxiety and depression.
While I knew my overall health wasn’t excellent, I still considered myself to be in good health. I was a full-time student at the University of Michigan, double majoring in Spanish Language & Literature and Environmental Health, with a specialization in Conservation Biology. I worked part-time to help cover the financial gaps in my educational expenses. I was a five-time All-American Runner at the National Intercollegiate Running Club Association (2012-14) and co-captain of the Michigan Running Club where I coached my Track & Field team to compete at Club and Varsity (Division I and II) meets. I also organized fundraising events for Relay for Life, My Team Triumph, and the Special Olympics every year.
Because I was able to achieve whatever I sought to do, I put my health on the back burner and suffered greatly because of it. Behind closed doors, I let fear take over control. Deep down, I knew everything I had worked so hard for could come to an end with one wrong swallow. The dread was amplified during times of stress, which, again, reminded me that no one knew how to help. It was a vicious cycle and positive feedback loop I needed to break from if I wanted to truly be free. I felt as if I was a mystery to myself.
That is, until I started to do some research …
EoE presents with a heterogeneity of mixed endoscopic appearances, with the co-existence of inflammation, ineffective contractile patterns, and fibrotic and pressure abnormalities. These attributes are more commonly observed than a strictly defined EoE subtype (Hirano et al., 2013). The chief pathophysiological mechanism behind EoE does not appear to be a strict IgE-mediated allergic response but rather a delayed hypersensitivity reaction to exceedingly common and regularly eaten foods (Lucendo & Lucendo, 2010). With a symptomatic response rate ranging from 70% to 96% (Kelly et al., 1995; Liacouras et al., 2005; Spergel et al., 2005, 2012; Kagalwalla et al., 2006; Gonsalves et al., 2012; Henderson et al., 2012; Lucendo et al., 2013) and with comparable efficacy to topically swallowed steroids (Liacouras et al., 2011), elimination diet therapy is the gold standard treatment in EoE (Table 1).
But elimination diet therapy is not 100% effective. Some evidence supports aeroallergens in the etiology of EoE (Moawad et al., 2010), while other evidence refutes the theory (Lucendo et al., 2015). Due to the conflicting nature of these results, the search for increasing efficacy in EoE continues.
Antecedents of Disease, The Hygiene Hypothesis and Sex:
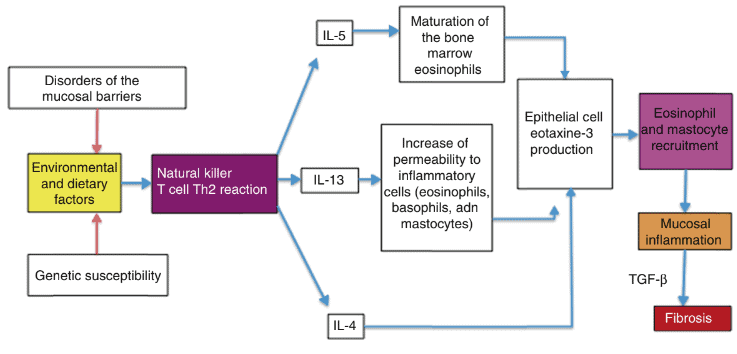
Given that the prevalence of EoE is increasing in developed countries, the hygiene hypothesis, considered heavily in atopic diseases, with which EoE is associated, takes center stage. The hygiene hypothesis is rooted in the idea that microbial exposure in early life fosters immune system tolerance. A dearth of pathogenic exposure in early life, on the other hand, disables the immune system’s tolerability, so much so that it increases one’s susceptibility to allergic diseases (García-Compeán et al., 2017). The interplay of the mucosal surface of the GI tract and the microbiota functions like a standalone organ in host defense. With the immune system built on an unsteady foundation–a foundation lacking early life exposures to microbial pathogens–, a defect is veritably imprinted on the immune system. The reprogrammed immune system in the GI tract shifts towards a Th2–an IL-4-, IL-5-, and IL-13-mediated–phenotypic expression.
The commensal microflora are implicated here. This may be why EoE is nonexistent in Africa. EoE is documented in every continent except Africa (Rodrigues et al., 2013). If the immune system were designed to be stimulated by certain bacteria and viruses (a Th1 response), then researchers and practitioners have to question the consequences of a non-stimulated immune system. For some individuals, the result appears to be atopic disorders. Tolerance defects likely include Caesarian sections, lack of breastfeeding, stay in neonatal intensive care units, or antibiotic use. Each of these exposures may increase risk of EoE (Jensen et al., 2018). Despite all these microbiome-altering experiences and their implication in EoE development, no direct or causative relationships have been found to date. It seems prudent, though, to increase beneficial probiotic strains that not only decrease esophageal inflammation but drive Treg upregulation, thereby balancing Th1 and Th2 immune responses.
Esophageal Permeability & Dietary Triggers:
Histologically, dilated intercellular spaces (or spongiosis) is a common finding in EoE, suggestive of a permeable esophageal barrier due to the enhanced breakdown of junction proteins (Collins, 2008), likely due to the defense and repair process of the esophagus (e.g., the immune system) already mentioned. If inflammatory mediators induce tissue damage, then the structural integrity of the esophagus (e.g. the epithelial cell) has to be implicated in the development of EoE, too. In an ideal state, esophageal epithelial cells are joined together by tight junction proteins, adherens junctions, and desmosomes, which are made up of essential proteins claudin-1 and -4, E-cadherin, and desmoglein (Orlando, 2010). A major defect in barrier function could allow for the passage of luminal antigens into esophageal tissue, thereby initiating a histologic and symptomatic response characteristic of EoE. Because barrier proteins like eotaxin-3 are differentially expressed in EoE (induced by the presence of IL-13), suppressing the inflammatory signaling molecules may directly impact cell barrier function and disease improvement (Blanchard et al., 2006). One supplement that could increase structural integrity of the GI tract is zinc carnosine (ZnC), a synthetically produced crystalline chelate containing L-carnosine and zinc. ZnC quickens the gut repair processes (migration and proliferation of cells) and stabilizes GI mucosal integrity in a dose-dependent manner. ZnC also decreases gastric (75% reduction at 5 mg/ml) and small bowel injury (50% reduction in villus shortening at 40 mg/ml, both p < 0.01) (Mahmood et al., 2007).
Table 1 provides a list of novel anti-inflammatory agents that should be considered in EoE. In addition to ZnC, quercetin, a plant flavonol (from the flavonoid group of polyphenols) found in many fruits, vegetables, leaves, and grains, is a powerful antioxidant. Quercetin may be indicated in EoE because of its ability to 1.) act as an antioxidant in free radical scavenging and 2.) decrease allergic responses by inhibiting pro-inflammatory cytokines like IL-4, histamine release, leukotriene synthesis, and other inflammatory mediators (Mlcek, Jurikova, Skrovankova, & Sochor, 2016). Because quercetin is both anti-allergic and anti-inflammatory, supplementation in EoE could lead to a dramatic improvement with dietary intervention. Furthermore, quercetin can improve the Th1/Th2 balance, and even inhibit antigen-specific IgE antibody formation and enzymes like lipoxygenase and eosinophil peroxidase (Mlcek, Jurikova, Skrovankova, & Sochor, 2016). Red onions, broccoli, kale, grapes, apples, berries, and some herbs like Ginkgo biloba and St. John’s wort host appreciable amounts of quercetin.
Keeping these two nutraceuticals in mind, another observed phenomena is the underexpression of filaggrin (In addition to IL-13–mediated epithelial cell response triggering eotaxin-3 overproduction) in EoE (Blanchard et al., 2010). Underexpression of filaggrin may contribute to a permeable epithelial barrier, where antigens can more easily penetrate. The principle function of filaggrin is to aggregate the epidermal cytoskeleton to create a dense lipid-protein matrix, thereby tightly regulating permeability of the skin to both water and aeroallergens (Jensen et al., 2004). A deficiency in filaggrin expression likely results from the inheritance of two loss-of-function allelic variants, 2282del4 and R510X. Decreased filaggrin concentrations support the theory that significant overlap exists between the mucosal structure of the skin and the mucosal structure of the esophagus (Blanchard et al., 2010). The similarities give support for why EoE is strongly associated with atopic disorders (Roy–Ghanta et al., 2008). When antigens cross this barrier in a susceptible individual, both eosinophils and esophageal epithelial cells can present antigen (Le-Carlson et al., 2013). In mice deficient in filaggrin, skin is abnormally permeable to environmental antigens (Fallon et al., 2009), which implicates filaggrin deficiency in inflammatory skin disease and allergic conditions like eczema, asthma and/or hay fever (Sandilands et al., 2007; Brown et al., 2008; Henderson et al., 2008; Weidinger et al., 2008).
Chromosome 1, home to several epidermal differentiation complex genes responsible for epithelial tissue growth and repair, is the most significantly modified chromosome (p = 0.0002) in EoE. FLG is the gene located on chromosome 1q21 that has all the instructions to make flaggrin (Marenholz et al., 1996). A majority of the genes on chromosome 1q21 have decreased expressions; filaggrin, in particular, is downregulated 16-fold in EoE relative to healthy controls (Blanchard et al., 2010). Chromosome 1q21 is also a known region associated with atopy (Sharma et al., 2007), where a defect in synthesis of barrier proteins–designed to protect the body from the outside world–manifests as a disease where the patient becomes reactive to the world.
Yet, the human genome alone is not enough to explain the rise in primary allergic etiology and EoE over the past few decades (Giriens et al., 2015). With this understanding, EoE can be traced back to the cell; it is a cellular disease of impaired barrier function in an acidic environment of inflammatory mediators and positive feedback mechanisms that provoke ongoing symptoms. Despite a genetic propensity, many strides can be made from an alkaline, anti-inflammatory diet alone. From a physiological perspective, organ systems like the esophagus operate within specific pH ranges. Achieving an acid-alkaline balance is required in EoE, and general recommendations are provided in Table 1. (Notice the striking similarities between elimination diet therapies and an alkaline diet.) Since an acidic pH increases cellular eotaxin-3, which is associated with increased severity of eosinophilia (Blanchard et al., 2010), the removal of acidic foods from the diet (e.g. grain, egg, fish, meat, and dairy products) can positively impact histologic and symptomatic presentation (Table 1). This is a revolutionary, non-allergen perspective of EoE. Acidity begets allergenicity, which better explains the enigma of EoE. It’s not one or the other–both are uniquely linked.
Mediators of Disease, Th2-derived IL-4, IL-5, & IL-13.
As previously mentioned, human and murine EoE models demonstrate an inflammatory signaling profile that’s Th2-dominant (Mishra & Rothenberg, 2003). Chemical signaling molecules, called cytokines, pertinent to the Th2 response include IL-4, IL-5, and IL-13. EoE is associated with an increase in all three Th2 cytokines (Blanchard, & Rothenberg, 2005). In fact, humanized neutralizing antibodies against human IL-5 (mepolizumab or “anti-IL-5”) was effective in reducing tissue eosinophil levels and improving HRQoL measurements in an open-label trial (Garrett et al., 2004). IL-5 regulates a host biological mechanisms associated with eosinophils including bone marrow release of eosinophils, eosinophil tissue survival, eosinophil activation, and antigen-induced eosinophilia (Gleich, 2000).
Of the three cytokines, though, IL-13 is the major mediator in EoE, as esophageal epithelial cells express all components of the IL-13 receptor including IL-4Rα, IL13Rα1, and IL-13Rα2 (Blanchard et al., 2007). IL-13 switches on the CCL26 gene to synthesize eotaxin-3, which is overexpressed in vivo in the esophageal transcriptome of EoE (Blanchard et al., 2007). Eosinophils, basophils, mast cells, lymphocytes, and smooth muscle cells make up the inflammatory infiltrate because they are dynamic IL-13–generating cells (Yamazaki et al., 2006). The dominance of these three cytokines is a key reason why esophageal tissue in EoE differs from healthy controls: Th2 cytokines change cellular protein synthesis. While there is extensive lamina propria remodeling, likely involving fibroblasts, epithelial cell hyperplasia, and elongation of the papillae (endothelial cells and fibroblasts) (Sant’Anna et al., 2004; Blanchard, Wang, & Rothenberg, 2006; Parfitt et al., 2006), the abnormal accumulation of eosinophils, mast cells (Blanchard et al., 2005; Kirsch et al., 2007), and lymphocytes (Straumann et al., 2002; Blanchard et al., 2005) is most striking because it irrevocably changes the cellular environment to one of inflammation. Thus, anti-IL-4, -IL-5, and -IL-13 therapies are all necessitated in EoE (Figure 7).
EoE, like atopic diseases, demonstrate a faulty immune system ill-prepared to find homeostatic expression (Th1-Th2 harmonization) in an ever-changing milieu of microbial and environmental inputs. This may be why an inverse relationship between EoE and Helicobacter pylori in developed countries has been documented and validated across distinct populations (Furuta et al., 2013). Interferon gamma (IFN-γ) and IL-17, two other major cytokines of the immune system, are expressed after contact with H. pylori virulence factors (Shi et al., 2010). H. pylori residence results in the proliferation of Th1 and Th17 cells, respectively, which subsequently downregulates atopy-associated Th2 cells. Shifting from an overactive Th2 state to Th1 could possibly check H. pylori residence could halt EoE disease presentation simply because Th1 and Th2 cellular responses, acting as a system of checks and balances, cannot occur at the same time.
Even though the rising prevalence of EoE and slight decline of H. pylori correlate inversely, no human data exists at present to indicate a causal effect. If this were true, however, then the eradication of H. pylori may not necessarily be an end goal for EoE patients who are already in a state of immune system dysregulation. The best supportive evidence comes from atopic disease (e.g. Th2) studies in animals, where H. pylori has a direct and protective effect due to dendritic cell-derived Treg differentiation (Arnold et al., 2011; Oertli et al., 2012). Tregs help balance the Th1-Th2-teeter totter. Hence, driving Tregs would theoretically be an effective anti-IL-4, -IL-5, and -IL-13 therapy. Diet, specific probiotic strains, Vitamin A and D, meditation, and yoga can all drive a Treg response, holistically treating inflammatory cytokines (Table 1).
Probiotic Strain Specificity: Future Treatments?
While we are a long way from understanding the importance of the esophageal microbiome in EoE, specific probiotic strains have been extensively used in various allergy models, providing health benefits that range from gut comfort to reduction or prevention of allergic symptoms (Cuello-Garcia et al., 2015), especially in decreasing airway inflammation (Feleszko et al., 2007; Pellaton et al., 2012) and preventing atopic dermatitis (Inoue et al., 2007; Kawashima et al., 2008; Won et al., 2011).
Holvoet et al. (2015) identified a specific probiotic strain, Lactococcus lactis NCC 2287, that significantly curbed esophageal eosinophilic inflammation, but in their preclinical model of EoE, this effect was dependent on the timing and duration of supplementation. Both L. lactis NCC 2287 and B. lactis NCC 2818 induce high concentrations of the anti-inflammatory associated cytokine, IL-10, in a Th2-skewed peripheral blood mononuclear cell (PBMC) model, suggesting an immunoregulatory effect (Holvoet et al., 2013). Theoretically, these bacterial strains appear to aid in the shift away from the overactive Th2 response in EoE (Table 1). Mechanistic actions of L. lactis NCC 2287 on allergic inflammation are unclear, but probiotics, as a class, are thought to 1.) increase the CD4+CD25+Foxp3+ regulatory T cells, which are known to contribute to peripheral immune tolerance (Kim et al., 2014; Wu et al., 2016), 2.) decrease sensitization efficacy (Feleszko et al., 2007; Pellaton et al., 2012), and 3.) modulate cytokine expression (Oliveira et al., 2011). Some probiotics have been shown to even stabilize IL-10 mRNA expression in human monocyte ex vivo (Demont et al., 2016). Tregs are associated with decreased esophageal eosinophilia in EoE (Dioszeghy et al., 2014), which would lead to greater tolerance of environmental inputs (Table 1).
When we understand byproducts of probiotic bacterial strains, the beneficial effects make sense. One of the key compounds produced by a healthy microbiome is butyrate, a short chain fatty acid (SCFA). Clostridia clusters XIVa and IV, for example, are made up of very diverse bacterial species, many of which are categorized by their ability to synthesize butyrate (Sokol et al., 2008). Butyrate is involved in colonic epithelium homeostasis and initiating anti-inflammatory responses (Joossens et al., 2011). In this way, butyrate signals colonic regulatory Treg induction (Smith et al, 2013). Miyake et al. (2015) found a striking depletion of Clostridia XIVa and IV clusters and argue that such a dramatic drop in a large subset of clostridial (butyrate-producing) microorganisms is implicated in the development of diseases like multiple sclerosis (Table 1).
Probiotic strain specificity likely directs the host’s immune response in the esophagus. This is the critical epigenetic component of EoE. Appreciation of the bacterial communities present may offer unique therapeutic strategies to impact EoE. Decreasing gram-negative bacteria, may reduce systemic lipopolysaccharide (LPS) concentrations. LPS is known to increase intestinal tight junction permeability in vitro and in vivo (by inducing enterocyte expression/localization of TLR-4 and CD14) (Guo, Al-Sadi, Said, & Ma, 2013). Probiotics likely help by (selectively) modifying the GI ecosystem, stimulating the migrating motor complex (MMC), and helping heal leaky epithelial barriers. Bifidobacterium, Lactococcus, and Clostridia clusters XIVa and IV supplementation may be the very first step at partially restoring normal intestinal microecology and increasing prokinetic action (i.e. inducing the MMC in human GI tract). Large-scale, longitudinal studies will help explain the nuances in the diseased-state microbiome, delineate the effect of the immune system upon changes in microbial composition, and provide personalized, strain-specific treatment options to EoE patients. Of course, the aforementioned therapies form the periphery of the EoE treatment page; non-antigenic, alkaline dietary interventions form the center.
Table 1. Nutritional & Lifestyle Recommendations to Improve EoE: Component of Tomorrow’s Treatment?
| Potential Therapeutic Modalities for EoE | Supporting Theoretical Evidence |
| Removal of acidic and allergenic foods (i.e Elimination Diet Therapy) | Foods are the major triggering agent in EoE. Soy, cow’s milk protein, wheat, eggs, fish/shellfish, and peanuts/tree nuts must be removed. Animal proteins and cereal grains are broken down to acidic residues, mainly sulfuric acid, which can progress to a chronic low-grade level of metabolic acidosis. The modern SAD is highly acidogenic, generating 75–100 mEq acid per day (Lemann Jr, 1999). Shifting away from an acidic diet should decrease eotaxin-3, thereby decreasing the severity of eosinophilia (Blanchard et al., 2010). |
| Removal of alcoholic beverages | Alcohol applies the brakes to the GI system; it causes impaired esophageal motility and transient lower esophageal relaxations, and slows gastric emptying but increases gastric acid secretion (Mayer, Grabowski, & Fisher, 1978). Having this system stall when swallowing foods is what EoE patients experience during dramatic events like food impaction. |
| Inclusion of alkaline foods | Fruit and vegetables are metabolized to alkaline residues, mainly potassium bicarbonate (Lemann Jr, 1999). Plant-based meals do not contribute to an acidic milieu as much; additional support may be provided from a fat-soluble extract containing chlorophyll. Liquid chlorophyll could theoretically coat an inflamed esophagus and alter the pH overtime to a less acidic state. This may theoretically reduce eotaxin-3 and the severity of eosinophilia (Blanchard et al., 2010). |
| Anti-inflammatory agents | ZnC prevents gut permeability caused by NSAIDs (Mahmood et al., 2007); quercetin is a powerful anti-inflammatory and immunomodulating agent (Mlcek et al., 2016); Deglycyrrhizinated liquorice (DGL) root extract increases mucosal production and blood supply to damaged sections of the GI tract, thereby enhancing epithelium healing (Van Marle et al, 1981); Vitamin A and E, glutathione, melatonin, N-acetylcysteine, selenium, CoQ10, and ellagic acid (Myung et al., 2013); Vitamin C (Gil et al., 2002); Vitamin D (Smolders et al., 2009); Ginger and marshmallow extracts (Zaghlool et al., 2015); Nettle leaf (Kukrić et al., 2012); Slippery elm, fenugreek, devil’s claw, tormentil, Mexican yam, and wei tong ning, a traditional Chinese medicine (Langmead et al., 2002); Aloe vera (Hu et al., 2003); Tinospora cordifolia, Rubia cordifolia, and Fagonia cretica linn (Rawal et al., 2004). |
| Bifidobacterium lactis NCC 2818 | While Bifidobacterium lactis NCC 2818 did not reach statistical significance for reducing esophageal eosinophilia levels, Bifidobacterium species, in general, may help control inflammation by supporting Treg proliferation. Bifidobacterium species also increase the presence of transforming growth factor beta (TGF-β), a cytokine with Treg-like function (Zamani et al., 2016). In patients with psoriasis, for example, oral administration of B. infantis 35624 1×1010 CFU per day for 8 weeks likely results in reduced plasma CRP and TNF-α, compared to placebo, byway of TGF-β induction (Groeger et al., 2013). Exploration of therapeutic Bifidobacterium species warrants consideration as TGF-β can decrease intestinal tight junction permeability. |
| Lactococcus lactis NCC 2287 | Th2 cytokines that provoke EoE (IL-4, IL-5, and IL-13) would be regulated by a Th1 shift and concomitant increase in Treg expression. Thus, the counteracting effect of L. lactis NCC 2287 on IL-5 expression in Th2-skewed PBMCs (Holvoet et al., 2013) and on IL-13 expression in an ovalbumin/cholera toxin-induced food allergy model (Zuercher et al., 2011) explain the observed decrease in esophageal eosinophilia. L. lactis NCC 2287 is also a stronger inducer of IFN-γ and more potent in reducing the eosinophil survival cytokine IL-5 than B. lactis NCC 2818 (Holvoet et al., 2013). |
| Clostridia clusters XIVa and IV | Because Clostridia XIVa and IV clusters and Bacteroides fragilis can stimulate Foxp3+ Treg and suppress inflammation, reestablishing gut flora by correcting dysbiosis (which thereby alters the metabolism of the microbiome and positively impacts health) may be sought in the prevention and treatment of overt multiple sclerosis (Miyake et al., 2015). |
| Provide time for rest and relaxation | Yoga, meditation, and tai chi chuan exercises will all drive a Treg response (Yeh et al., 2006; Arora & Bhattacharjee, 2008). Eating slowly and thoroughly chewing food until it is fully masticated is important. Eating should be a relaxing experience, where one is mindful during the entire length of the meal. Food should not be consumed in an anxious or panicked state. Enhanced reactivity to even mildly psychological stress can initiate the release of cortisol, contributing to higher concentrations of proinflammatory cytokines (Kunz-Ebrecht et al., 2003). |
While my extraction of pertinent research studies was nowhere near fine-tuned, after searching for hours on the root causes of EoE I came to the conclusion that my diagnosis was likely diet related. Allergy testing confirmed it wasn’t in my head after all, and the antagonists were identified—9 food allergens I was consuming on a regular basis. After pinpointing the specific food triggers with the allergist, when I requested a tailored nutrition plan and guidance for the next steps, I was quickly written off with “Google it” as the response from my doctor. His back was turned to me. He didn’t even look up from his prescription pad when he said it and walked out the door.
So I did.
The truth is modern medicine failed me and, arguably, the food system and my upbringing. My mother was told infant formula was better. Placed on several different drugs to treat several different symptoms continued to mask the underlying cause for two decades: the food I was eating. Inflammation ran rampant in my system and conventional drugs were wreaking havoc in my gut. No one warned me of the potential side effects or invited me to question if there could be a connection between all my underlying health issues.
Conclusion
Tempestuous and destructive are words that describe the immune system’s mercurial-like nature in the esophagus of patients with EoE. If the thalamus is the central processing unit of the brain, the esophagus is the central food monitor, immediately accepting or rejecting the passage of dietary constituents. We are at the veritable tip of the iceberg when it comes to understanding EoE, for which dysphagia is literally at the heart. Clinical experience, decades of research, and time-tested trial and error strategies demonstrate that food allergens are the number one trigger in EoE, for which elimination diet therapies are the number one treatment option. Still, EoE has a multifactorial pathogenesis and multiple novel treatment modalities must be pursued that go beyond diet and pharmacy. Alternative recommendations to improve symptomatic and histologic parameters include chlorophyll-rich foods that are not antigenic to the individual, ZnC, quercetin, Vitamins A, C, and D, deglycyrrhizinated liquorice, and specific probiotic strains, all of which should coat the inflamed organ. Stress reduction (i.e. yoga, meditation, tai chi chuan) practices and eating slowly and mindfully during mealtime is beyond warranted.
References
Arnold, I. C., Dehzad, N., Reuter, S., Martin, H., Becher, B., Taube, C., & Müller, A. (2011). Helicobacter pylori infection prevents allergic asthma in mouse models through the induction of regulatory T cells. The Journal of clinical investigation, 121(8), 3088-3093. Retrieved from: https://www.jci.org/articles/view/45041/pdf
Arora, S., & Bhattacharjee, J. (2008). Modulation of immune responses in stress by Yoga. International journal of yoga, 1(2), 45. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3144610/
Blanchard, C., Durual, S., Estienne, M., Emami, S., Vasseur, S., & Cuber, J. C. (2005). Eotaxin-3/CCL26 gene expression in intestinal epithelial cells is up-regulated by interleukin-4 and interleukin-13 via the signal transducer and activator of transcription 6. The international journal of biochemistry & cell biology, 37(12), 2559-2573. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S1357272505001962&site=eds-live&scope=site
Blanchard, C., Mingler, M. K., Vicario, M., Abonia, J. P., Wu, Y. Y., Lu, T. X., … & Rothenberg, M. E. (2007). IL-13 involvement in eosinophilic esophagitis: transcriptome analysis and reversibility with glucocorticoids. Journal of Allergy and Clinical Immunology, 120(6), 1292-1300. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=18073124&site=eds-live&scope=site
Blanchard, C., & Rothenberg, M. E. (2008). Basic pathogenesis of eosinophilic esophagitis. Gastrointestinal endoscopy clinics of North America, 18(1), 133-143. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2194642/
Blanchard, C., Stucke, E. M., Burwinkel, K., Caldwell, J. M., Collins, M. H., Ahrens, A., … & Franciosi, J. P. (2010). Coordinate interaction between IL-13 and epithelial differentiation cluster genes in eosinophilic esophagitis. The Journal of Immunology, ji_0903069. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=20208004&site=eds-live&scope=site
Blanchard, C., Wang, N., & Rothenberg, M. E. (2006). Eosinophilic esophagitis: pathogenesis, genetics, and therapy. Journal of allergy and clinical immunology, 118(5), 1054-1059. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.194647475&site=eds-live&scope=site
Blanchard, C., Wang, N., Stringer, K. F., Mishra, A., Fulkerson, P. C., Abonia, J. P., … & Cohen, M. B. (2006). Eotaxin-3 and a uniquely conserved gene-expression profile in eosinophilic esophagitis. The Journal of clinical investigation, 116(2), 536-547. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=16453027&site=eds-live&scope=site
Brown, S. J., Relton, C. L., Liao, H., Zhao, Y., Sandilands, A., Wilson, I. J., … & Cordell, H. J. (2008). Filaggrin null mutations and childhood atopic eczema: a population-based case-control study. Journal of Allergy and Clinical Immunology, 121(4), 940-946. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=18313126&site=eds-live&scope=site
Collins, M. H. (2008). Histopathologic features of eosinophilic esophagitis. Gastrointestinal endoscopy clinics of North America, 18(1), 59-71. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S0889855314000284&site=eds-live&scope=site
Cuello-Garcia, C. A., Brożek, J. L., Fiocchi, A., Pawankar, R., Yepes-Nuñez, J. J., Terracciano, L., … & Schünemann, H. J. (2015). Probiotics for the prevention of allergy: a systematic review and meta-analysis of randomized controlled trials. Journal of Allergy and Clinical Immunology, 136(4), 952-961. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=26044853&site=eds-live&scope=site
Demont, A., Hacini-Rachinel, F., Doucet-Ladevèze, R., Ngom-Bru, C., Mercenier, A., Prioult, G., & Blanchard, C. (2016). Live and heat-treated probiotics differently modulate IL10 mRNA stabilization and microRNA expression. Journal of Allergy and Clinical Immunology, 137(4), 1264-1267. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=26478009&site=eds-live&scope=site
Dioszeghy, V., Mondoulet, L., Dhelft, V., Ligouis, M., Puteaux, E., Dupont, C., & Benhamou, P. H. (2014). The regulatory T cells induction by epicutaneous immunotherapy is sustained and mediates long‐term protection from eosinophilic disorders in peanut‐sensitized mice. Clinical & Experimental Allergy, 44(6), 867-881. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.369102962&site=eds-live&scope=site
Fallon, P. G., Sasaki, T., Sandilands, A., Campbell, L. E., Saunders, S. P., Mangan, N. E., … & Sundberg, J. P. (2009). A homozygous frameshift mutation in the mouse Flg gene facilitates enhanced percutaneous allergen priming. Nature genetics, 41(5), 602. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.199397091&site=eds-live&scope=site
Feleszko, W., Jaworska, J., Rha, R. D., Steinhausen, S., Avagyan, A., Jaudszus, A., … & Hamelmann, E. (2007). Probiotic‐induced suppression of allergic sensitization and airway inflammation is associated with an increase of T regulatory‐dependent mechanisms in a murine model of asthma. Clinical & Experimental Allergy, 37(4), 498-505. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=17430345&site=eds-live&scope=site
Furuta, K., Adachi, K., Aimi, M., Ishimura, N., Sato, S., Ishihara, S., & Kinoshita, Y. (2013). Case-control study of association of eosinophilic gastrointestinal disorders with Helicobacter pylori infection in Japan. Journal of clinical biochemistry and nutrition, 53(1), 60-62. Retrieved from: https://www.jstage.jst.go.jp/article/jcbn/53/1/53_13-15/_pdf
García-Compeán, D., González-González, J. A., González-Moreno, E. I., & Maldonado-Garza, H. J. (2017). Eosinophilic esophagitis. The North against the South? A bio-economic-social mechanistic approach and clinical implications. Revista de Gastroenterología de México (English Edition), 82(4), 328-336. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=28676192&site=eds-live&scope=site
Garrett, J. K., Jameson, S. C., Thomson, B., Collins, M. H., Wagoner, L. E., Freese, D. K., … & Sutton, S. A. (2004). Anti–interleukin-5 (mepolizumab) therapy for hypereosinophilic syndromes. Journal of Allergy and Clinical Immunology, 113(1), 115-119. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S0091674903025338&site=eds-live&scope=site
Gil, M. I., Tomás-Barberán, F. A., Hess-Pierce, B., & Kader, A. A. (2002). Antioxidant capacities, phenolic compounds, carotenoids, and vitamin C contents of nectarine, peach, and plum cultivars from California. Journal of Agricultural and Food Chemistry, 50(17), 4976-4982. Retrieved from: https://ucanr.edu/datastoreFiles/234-25.pdf
Giriens, B., Yan, P., Safroneeva, E., Zwahlen, M., Reinhard, A., Nydegger, A., … & Schoepfer, A. M. (2015). Escalating incidence of eosinophilic esophagitis in Canton of Vaud, Switzerland, 1993–2013: a population‐based study. Allergy, 70(12), 1633-1639. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edb&AN=111310497&site=eds-live&scope=site
Gleich, G. J. (2000). Mechanisms of eosinophil-associated inflammation. Journal of Allergy and Clinical Immunology, 105(4), 651-663. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.290798727&site=eds-live&scope=site
Gonsalves, N., Yang, G. Y., Doerfler, B., Ritz, S., Ditto, A. M., & Hirano, I. (2012). Elimination diet effectively treats eosinophilic esophagitis in adults; food reintroduction identifies causative factors. Gastroenterology, 142(7), 1451-1459. Retrieved from: https://www.gastrojournal.org/article/S0016-5085(12)00309-5/fulltext
Groeger, D., O’Mahony, L., Murphy, E. F., Bourke, J. F., Dinan, T. G., Kiely, B., … & Quigley, E. M. (2013). Bifidobacterium infantis 35624 modulates host inflammatory processes beyond the gut. Gut Microbes, 4(4), 325-339. Retrieved from: https://www-ncbi-nlm-nih-gov.uws.idm.oclc.org/pmc/articles/PMC3744517/
Guo, S., Al-Sadi, R., Said, H. M., & Ma, T. Y. (2013). Lipopolysaccharide causes an increase in intestinal tight junction permeability in vitro and in vivo by inducing enterocyte membrane expression and localization of TLR-4 and CD14. The American journal of pathology, 182(2), 375-387. Retrieved from: https://www.sciencedirect.com/science/article/pii/S0002944012008085
Henderson, C. J., Abonia, J. P., King, E. C., Putnam, P. E., Collins, M. H., Franciosi, J. P., & Rothenberg, M. E. (2012). Comparative dietary therapy effectiveness in remission of pediatric eosinophilic esophagitis. Journal of Allergy and Clinical Immunology, 129(6), 1570-1578. Retrieved from: https://www.jacionline.org/article/S0091-6749(12)00528-3/fulltext
Henderson, J., Northstone, K., Lee, S. P., Liao, H., Zhao, Y., Pembrey, M., … & Irvine, A. D. (2008). The burden of disease associated with filaggrin mutations: a population-based, longitudinal birth cohort study. Journal of Allergy and Clinical Immunology, 121(4), 872-877. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=18325573&site=eds-live&scope=site
Hirano, I., Moy, N., Heckman, M. G., Thomas, C. S., Gonsalves, N., & Achem, S. R. (2013). Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut, 62(4), 489-495. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.321806058&site=eds-live&scope=site
Holvoet, S., Zuercher, A. W., Julien-Javaux, F., Perrot, M., & Mercenier, A. (2013). Characterization of candidate anti-allergic probiotic strains in a model of Th2-skewed human peripheral blood mononuclear cells. International archives of allergy and immunology, 161(2), 142-154. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=23343780&site=eds-live&scope=site
Homan, M., Blagus, R., Jeverica, A. K., & Orel, R. (2015). Pediatric eosinophilic esophagitis in Slovenia: data from a retrospective 2005–2012 epidemiological study. Journal of pediatric gastroenterology and nutrition, 61(3), 313-318. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=26020481&site=eds-live&scope=site
Hu, Y., Xu, J., & Hu, Q. (2003). Evaluation of antioxidant potential of Aloe vera (Aloe barbadensis Miller) extracts. Journal of agricultural and food chemistry, 51(26), 7788-7791. Retrieved from: www.sld.cu/galerias/pdf/sitios/mednat/actividad_antioxidante_del_aloe_vera.pdf
Inoue, R., Nishio, A., Fukushima, Y., & Ushida, K. (2007). Oral treatment with probiotic Lactobacillus johnsonii NCC533 (La1) for a specific part of the weaning period prevents the development of atopic dermatitis induced after maturation in model mice, NC/Nga. British Journal of Dermatology, 156(3), 499-509. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.159642165&site=eds-live&scope=site
Jensen, E. T., Kuhl, J. T., Martin, L. J., Rothenberg, M. E., & Dellon, E. S. (2018). Prenatal, intrapartum, and postnatal factors are associated with pediatric eosinophilic esophagitis. Journal of Allergy and Clinical Immunology, 141(1), 214-222. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S009167491730917X&site=eds-live&scope=site
Jensen, J. M., Fölster-Holst, R., Baranowsky, A., Schunck, M., Winoto-Morbach, S., Neumann, C., … & Proksch, E. (2004). Impaired sphingomyelinase activity and epidermal differentiation in atopic dermatitis. Journal of Investigative Dermatology, 122(6), 1423-1431. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=15175033&site=eds-live&scope=site
Joossens, M., Huys, G., Cnockaert, M., De Preter, V., Verbeke, K., Rutgeerts, P., … & Vermeire, S. (2011). Dysbiosis of the faecal microbiota in patients with Crohn’s disease and their unaffected relatives. Gut, 2011. Retrieved from: https://gut-bmj-com.uws.idm.oclc.org/content/60/5/631.full
Kagalwalla, A. F., Sentongo, T. A., Ritz, S., Hess, T., Nelson, S. P., Emerick, K. M., … & Li, B. U. K. (2006). Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clinical gastroenterology and hepatology, 4(9), 1097-1102. Retrieved from: https://www.cghjournal.org/article/S1542-3565(06)00495-2/pdf
Kawashima, H., Tateishi, N., Shiraishi, A., Teraoka, N., Tanaka, T., Tanaka, A., … & Kiso, Y. (2008). Oral Administration of Dihomo‐γ‐Linolenic Acid Prevents Development of Atopic Dermatitis in NC/Nga Mice. Lipids, 43(1), 37-43. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edb&AN=49684497&site=eds-live&scope=site
Kelly, K. J., Lazenby, A. J., Rowe, P. C., Yardley, J. H., Perman, J. A., & Sampson, H. A. (1995). Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology, 109(5), 1503-1512. Retrieved from: https://www.gastrojournal.org/article/0016-5085(95)90637-1/pdf
Kim, H. J., Kim, Y. J., Lee, S. H., Yu, J., Jeong, S. K., & Hong, S. J. (2014). Effects of Lactobacillus rhamnosus on allergic march model by suppressing Th2, Th17, and TSLP responses via CD4+ CD25+ Foxp3+ Tregs. Clinical Immunology, 153(1), 178-186. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S1521661614001156&site=eds-live&scope=site
Kirsch, R., Bokhary, R., Marcon, M. A., & Cutz, E. (2007). Activated mucosal mast cells differentiate eosinophilic (allergic) esophagitis from gastroesophageal reflux disease. Journal of pediatric gastroenterology and nutrition, 44(1), 20-26. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=17204948&site=eds-live&scope=site
Kukrić, Z. Z., Topalić-Trivunović, L. N., Kukavica, B. M., Matoš, S. B., Pavičić, S. S., Boroja, M. M., & Savić, A. V. (2012). Characterization of antioxidant and antimicrobial activities of nettle leaves (Urtica dioica L.). Apteff, 43, 1-342. Retrieved from: www.japsonline.com/admin/php/uploads/904_pdf.pdf
Kunz-Ebrecht, S. R., Mohamed-Ali, V., Feldman, P. J., Kirschbaum, C., & Steptoe, A. (2003). Cortisol responses to mild psychological stress are inversely associated with proinflammatory cytokines. Brain, behavior, and immunity, 17(5), 373-383. Retrieved from: citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.460.7473&rep=rep1&type=pdf
Langmead, L., Dawson, C., Hawkins, C., Banna, N., Loo, S., & Rampton, D. S. (2002). Antioxidant effects of herbal therapies used by patients with inflammatory bowel disease: an in vitro study. Alimentary pharmacology & therapeutics, 16(2), 197-205. Retrieved from: https://onlinelibrary.wiley.com/doi/epdf/10.1046/j.1365-2036.2002.01157.x
Le-Carlson, M., Seki, S., Abarbanel, D., Quiros, A., Cox, K., & Nadeau, K. C. (2013). Markers of antigen presentation and activation on eosinophils and T cells in the esophageal tissue of patients with eosinophilic esophagitis. Journal of pediatric gastroenterology and nutrition, 56(3), 257. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=23059644&site=eds-live&scope=site
Lemann Jr, J. (1999). Relationship between urinary calcium and net acid excretion as determined by dietary protein and potassium: a review. Nephron, 81(Suppl. 1), 18-25. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edb&AN=11441538&site=eds-live&scope=site
Liacouras, C. A., Furuta, G. T., Hirano, I., Atkins, D., Attwood, S. E., Bonis, P. A., … & Dohil, R. (2011). Eosinophilic esophagitis: updated consensus recommendations for children and adults. Journal of Allergy and Clinical Immunology, 128(1), 3-20. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=21477849&site=eds-live&scope=site
Liacouras, C. A., Spergel, J. M., Ruchelli, E., Verma, R., Mascarenhas, M., Semeao, E., … & Markowitz, J. E. (2005). Eosinophilic esophagitis: a 10-year experience in 381 children. Clinical Gastroenterology and Hepatology, 3(12), 1198-1206. Retrieved from: https://www.cghjournal.org/article/S1542-3565(05)00885-2/fulltext
Lucendo, A. J., Arias, Á., González-Cervera, J., Yagüe-Compadre, J. L., Guagnozzi, D., Angueira, T., … & Tenias, J. M. (2013). Empiric 6-food elimination diet induced and maintained prolonged remission in patients with adult eosinophilic esophagitis: a prospective study on the food cause of the disease. Journal of Allergy and Clinical Immunology, 131(3), 797-804. Retrieved from: https://www.jacionline.org/article/S0091-6749(12)02644-9/fulltext
Lucendo, A. J., Arias, Á., Redondo‐González, O., & González‐Cervera, J. (2015). Seasonal distribution of initial diagnosis and clinical recrudescence of eosinophilic esophagitis: a systematic review and meta‐analysis. Allergy, 70(12), 1640-1650. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=26392117&site=eds-live&scope=site
Lucendo, A. J., & Lucendo, B. (2010). An update on the immunopathogenesis of eosinophilic esophagitis. Expert review of gastroenterology & hepatology, 4(2), 141-148. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.222460364&site=eds-live&scope=site
Mahmood, A., Fitzgerald, A. J., Marchbank, T., Ntatsaki, E., Murray, D., Ghosh, S., & Playford, R. J. (2007). Zinc carnosine, a health food supplement that stabilises small bowel integrity and stimulates gut repair processes. Gut, 56(2), 168-175. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1856764/?__hstc=209342221.eb264583e30de5d421a6215b1d361d56.1464825600047.1464825600048.1464825600049.1&__hssc=209342221.1.1464825600050&__hsfp=1314462730
Marenholz, I., Volz, A., Ziegler, A., Davies, A., Ragoussis, I., Korge, B. P., & Mischke, D. (1996). Genetic analysis of the epidermal differentiation complex (EDC) on human chromosome 1q21: chromosomal orientation, new markers, and a 6-Mb YAC contig. Genomics, 37(3), 295-302. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=8938441&site=eds-live&scope=site
Mishra, A., & Rothenberg, M. E. (2003). Intratracheal IL-13 induces eosinophilic esophagitis by an IL-5, eotaxin-1, and STAT6-dependent mechanism1. Gastroenterology, 125(5), 1419-1427. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edselp&AN=S0016508503013520&site=eds-live&scope=site
Miyake, S., Kim, S., Suda, W., Oshima, K., Nakamura, M., Matsuoka, T., … & Morita, H. (2015). Dysbiosis in the gut microbiota of patients with multiple sclerosis, with a striking depletion of species belonging to Clostridia XIVa and IV clusters. PLoS One, 10(9), e0137429. Retrieved from: https://www-ncbi-nlm-nih-gov.uws.idm.oclc.org/pmc/articles/PMC4569432/
Moawad, F. J., Veerappan, G. R., Lake, J. M., Maydonovitch, C. L., Haymore, B. R., Kosisky, S. E., & Wong, R. K. H. (2010). Correlation between eosinophilic oesophagitis and aeroallergens. Alimentary pharmacology & therapeutics, 31(4), 509-515. Retrieved from: https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2036.2009.04199.x
Myung, S. K., Ju, W., Cho, B., Oh, S. W., Park, S. M., Koo, B. K., & Park, B. J. (2013). Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: systematic review and meta-analysis of randomised controlled trials. Bmj, 346, f10. Retrieved from: https://onlinelibrary.wiley.com/doi/pdf/10.1002/ijc.23754
Oertli, M., Sundquist, M., Hitzler, I., Engler, D. B., Arnold, I. C., Reuter, S., … & Müller, A. (2012). DC-derived IL-18 drives Treg differentiation, murine Helicobacter pylori–specific immune tolerance, and asthma protection. The Journal of clinical investigation, 122(3), 1082-1096. Retrieved from: https://www.jci.org/articles/view/61029
Oliveira, M., Bosco, N., Perruisseau, G., Nicolas, J., Segura-Roggero, I., Duboux, S., … & Benyacoub, J. (2011). Lactobacillus paracasei reduces intestinal inflammation in adoptive transfer mouse model of experimental colitis. Clinical and Developmental Immunology, 2011. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=21808650&site=eds-live&scope=site
Orlando, R. C. (2010). The integrity of the esophageal mucosa. Balance between offensive and defensive mechanisms. Best practice & research Clinical gastroenterology, 24(6), 873-882. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.243650545&site=eds-live&scope=site
Parfitt, J. R., Gregor, J. C., Suskin, N. G., Jawa, H. A., & Driman, D. K. (2006). Eosinophilic esophagitis in adults: distinguishing features from gastroesophageal reflux disease: a study of 41 patients. Modern Pathology, 19(1), 90. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=16258505&site=eds-live&scope=site
Pellaton, C., Nutten, S., Thierry, A. C., Boudousquié, C., Barbier, N., Blanchard, C., … & Spertini, F. (2012). Intragastric and intranasal administration of Lactobacillus paracasei NCC2461 modulates allergic airway inflammation in mice. International journal of inflammation, 2012. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=22762009&site=eds-live&scope=site
Rawal, A. K., Muddeshwar, M. G., & Biswas, S. K. (2004). Rubia cordifolia, Fagonia cretica linn and Tinospora cordifolia exert neuroprotection by modulating the antioxidant system in rat hippocampal slices subjected to oxygen glucose deprivation. BMC complementary and alternative medicine, 4(1), 11. Retrieved from: https://bmccomplementalternmed.biomedcentral.com/articles/10.1186/1472-6882-4-11
Rodrigues, M., D’Amico, M. F. M., Patiño, F. R. A., Barbieri, D., Damião, A. O. M. C., & Sipahi, A. M. (2013). Clinical manifestations, treatment, and outcomes of children and adolescents with eosinophilic esophagitis. Jornal de pediatria, 89(2), 197-203. Retrieved from: www.scielo.br/scielo.php?script=sci_arttext&pid=S0021-75572013000200014&lng=en&nrm=iso&tlng=en
Roy–Ghanta, S., Larosa, D. F., & Katzka, D. A. (2008). Atopic characteristics of adult patients with eosinophilic esophagitis. Clinical Gastroenterology and Hepatology, 6(5), 531-535. Retrieved from: https://www.cghjournal.org/article/S1542-3565(07)01248-7/fulltext
Sandilands, A., Terron-Kwiatkowski, A., Hull, P. R., O’Regan, G. M., Clayton, T. H., Watson, R. M., … & Campbell, L. E. (2007). Comprehensive analysis of the gene encoding filaggrin uncovers prevalent and rare mutations in ichthyosis vulgaris and atopic eczema. Nature genetics, 39(5), 650. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.183393597&site=eds-live&scope=site
Sant’Anna, A. M. G. A., Rolland, S., Fournet, J. C., Yazbeck, S., & Drouin, E. (2004). Eosinophilic esophagitis in children: symptoms, histology and pH probe results. Journal of pediatric gastroenterology and nutrition, 39(4), 373-377. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=15448427&site=eds-live&scope=site
Sharma, M., Mehla, K., Batra, J., & Ghosh, B. (2007). Association of a chromosome 1q21 locus in close proximity to a late cornified envelope-like proline-rich 1 (LELP1) gene with total serum IgE levels. Journal of human genetics, 52(4), 378. Retrieved from: https://www.nature.com/articles/jhg200749.pdf
Shi, Y., Liu, X. F., Zhuang, Y., Zhang, J. Y., Liu, T., Yin, Z., … & Guo, H. (2010). Helicobacter pylori-induced Th17 responses modulate Th1 cell responses, benefit bacterial growth, and contribute to pathology in mice. The Journal of Immunology, 184(9), 1-9. Retrieved from: www.jimmunol.org/content/jimmunol/early/2010/03/29/jimmunol.0901115.full.pdf
Smith, P. M., Howitt, M. R., Panikov, N., Michaud, M., Gallini, C. A., Bohlooly-y, M., … & Garrett, W. S. (2013). The microbial metabolites, short-chain fatty acids, regulate colonic Treg cell homeostasis. Science, 341(6145), 569-573. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3807819/pdf/nihms-518169.pdf
Smolders, J., Thewissen, M., Peelen, E., Menheere, P., Tervaert, J. W. C., Damoiseaux, J., & Hupperts, R. (2009). Vitamin D status is positively correlated with regulatory T cell function in patients with multiple sclerosis. PloS one, 4(8), e6635. Retrieved from: https://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0006635&type=printable
Sokol, H., Pigneur, B., Watterlot, L., Lakhdari, O., Bermúdez-Humarán, L. G., Gratadoux, J. J., … & Grangette, C. (2008). Faecalibacterium prausnitzii is an anti-inflammatory commensal bacterium identified by gut microbiota analysis of Crohn disease patients. Proceedings of the National Academy of Sciences, 105(43), 16731-16736. Retrieved from: www.pnas.org/content/pnas/105/43/16731.full.pdf
Spergel, J. M., Andrews, T., Brown-Whitehorn, T. F., Beausoleil, J. L., & Liacouras, C. A. (2005). Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Annals of Allergy, Asthma & Immunology, 95(4), 336-343. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=16279563&site=eds-live&scope=site
Spergel, J. M., Brown-Whitehorn, T. F., Cianferoni, A., Shuker, M., Wang, M. L., Verma, R., & Liacouras, C. A. (2012). Identification of causative foods in children with eosinophilic esophagitis treated with an elimination diet. Journal of Allergy and Clinical Immunology, 130(2), 461-467. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=22743304&site=eds-live&scope=site
Straumann, A., Bauer, M., Fischer, B., Blaser, K., & Simon, H. U. (2002). Idiopathic eosinophilic esophagitis is associated with a T-helper 2-type allergic inflammatory response. Journal of Allergy and Clinical Immunology, 109(1), S225. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.290798849&site=eds-live&scope=site
Van Marle, J., Aarsen, P. N., Lind, A., & Van Weeren-Kramer, J. (1981). Deglycyrrhizinised liquorice (DGL) and the renewal of rat stomach epithelium. European journal of pharmacology, 72(2-3), 219-225.
Weidinger, S., O’sullivan, M., Illig, T., Baurecht, H., Depner, M., Rodriguez, E., … & McLean, W. I. (2008). Filaggrin mutations, atopic eczema, hay fever, and asthma in children. Journal of Allergy and Clinical Immunology, 121(5), 1203-1209. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=18396323&site=eds-live&scope=site
Won, T. J., Kim, B., Lim, Y. T., Song, D. S., Park, S. Y., Park, E. S., … & Hwang, K. W. (2011). Oral administration of Lactobacillus strains from Kimchi inhibits atopic dermatitis in NC/Nga mice. Journal of applied microbiology, 110(5), 1195-1202. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.253459306&site=eds-live&scope=site
Wu, C. T., Chen, P. J., Lee, Y. T., Ko, J. L., & Lue, K. H. (2016). Effects of immunomodulatory supplementation with Lactobacillus rhamnosus on airway inflammation in a mouse asthma model. Journal of Microbiology, Immunology and Infection, 49(5), 625-635. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=25440975&site=eds-live&scope=site
Yamazaki, K., Murray, J. A., Arora, A. S., Alexander, J. A., Smyrk, T. C., Butterfield, J. H., & Kita, H. (2006). Allergen-specific in vitro cytokine production in adult patients with eosinophilic esophagitis. Digestive diseases and sciences, 51(11), 1934-1941. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsgao&AN=edsgcl.154899785&site=eds-live&scope=site
Yeh, S. H., Chuang, H., Lin, L. W., Hsiao, C. Y., & Eng, H. L. (2006). Regular tai chi chuan exercise enhances functional mobility and CD4CD25 regulatory T cells. British journal of sports medicine, 40(3), 239-243. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2491999/
Zaghlool, S. S., Shehata, B. A., Abo-Seif, A. A., & El-Latif, H. A. A. (2015). Protective effects of ginger and marshmallow extracts on indomethacin-induced peptic ulcer in rats. Journal of natural science, biology, and medicine, 6(2), 421. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4518423/
Zamani, B., Golkar, H. R., Farshbaf, S., Emadi‐Baygi, M., Tajabadi‐Ebrahimi, M., Jafari, P., … & Asemi, Z. (2016). Clinical and metabolic response to probiotic supplementation in patients with rheumatoid arthritis: a randomized, double‐blind, placebo‐controlled trial. International journal of rheumatic diseases, 19(9), 869-879. Retrieved from: eds.b.ebscohost.com.uws.idm.oclc.org/eds/pdfviewer/pdfviewer?vid=2&sid=42505284-b97e-4c9a-b3aa-ae0fab99c20f%40sessionmgr101
Zuercher, A. W., Weiss, M., Holvoet, S., Moser, M., Moussu, H., Van Overtvelt, L., … & Singh, A. (2011). Lactococcus lactis NCC 2287 alleviates food allergic manifestations in sensitized mice by reducing IL-13 expression specifically in the ileum. Clinical and Developmental Immunology, 2012. Retrieved from: https://uws.idm.oclc.org/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mdc&AN=21961022&site=eds-live&scope=site
Related posts






HOW do you populate with those very specific probiotic strains, especially closdridia which I have never seen in a product.
Great question, since as you pointed out this isn’t found in a typical probiotic. It’s been proposed that the best way to facilitate the growth of a diverse species (in particular those indicated in certain illnesses) is to facilitate an environment that allows them to grow. That means approaching with a full FxMed approach which includes reducing exposures to any potential environmental triggers/antigens, eradicating any competing overgrowth or infection, balancing the pH of the GI, introducing diverse fiber/prebiotics, and maximizing polyphenols/phytonutrients. I should add that supporting proper eating habits – chewing, avoiding multitasking, and supporting exercise, sleep, and stress management must also be part of the comprehensive plan as these impact microbiome health as well.
Excellent! Thanks for sharing this important story.
Thank you so much for this amazing review of EOE. Do you know of any resources of recipes for people that need to follow this very restricted diet plan? Does someone need to continue this diet forever or could eventually reintroduce some foods. Do you recommend food sensitivity/allergy testing to help guide specific foods that could be problematic or just to avoid all foods on above list?
I would love to know a good diet resource for a healthy diet For a fussy child with EoE !! Other than leading a combination of a gluten free and vegan diet there is very few specific resources to ensure the essiential nutrients aren’t being missed out or recipes to support the body !! Help would be amazing
It can definitely be challenging with a picky eater, and likely some of the fussiness might be attributed to foods not feeling very good and a reluctance to try new things as a result. I would highly suggest working with a nutritionist who is well versed in EoE to identify the triggers and expand the diet accordingly while identifying any nutrient deficiencies that need to be addressed to prevent developmental delays or other complications.
In case you’re interested, the same author of this article also wrote another piece o his own experience you might find useful: https://www.drkarafitzgerald.com/2020/08/14/a-reckoning-with-modern-medicine-one-individuals-journey-to-find-healing-when-faced-with-eosinophilic-esophagitis/
Hi Katie,
Sorry for the delay. I thought this had been posted by the Lead Nutritionist! This is a wonderful question, and was top of my mind when I learned the role that food plays in EoE (5 years after my diagnosis). And you’re absolutely right about the diet being restrictive for a period of time. The truth is we need to consider: 1. healing the gut (and decreasing inflammation) and 2. providing recipes that are uniquely tailored to each person with EoE, since they do tend to vary from person to person. What I can say for certain is that there are six problematic foods commonly observed in EoE that need to be excluded for some time. In the EoE community, this is called the “Six Food Elimination Diet” or SFED for short. They include: cow-milk protein, soy, wheat, egg, peanut, and seafood. With the appropriate food sensitivity testing and patient identification of trigger foods, we can build upon that list while still providing healthy meal plans that work to heal the gastrointestinal tract. One need not continue the diet forever, as we typically do like to reintroduce foods and expand the diet as much as we can, but this varies case to case. Hence, we recommend running this trial and error process with a healthcare provider knowledgeable of food allergies/sensitivities for the best outcomes.
I so appreciate you shining a light on this challenging condition and getting education out there on how to recover from Eoe. As an acupuncturist and EoE sufferer (and recoverer!) I wanted to share this case study about using Chinese medicine to work EoE with your community. The more tools the better! https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7757072/?fbclid=IwAR0OU1ibDbVueaXvezt8IrlgdXR96QDoWXZSLBCsN7E4Ae3cFAm9DLDm5zo#!po=70.0000
Jeannie,
Thank you for sharing this research study! I look forward to discussing this information with future clients. As you know, EoE requires a holistic and individualized approach to treatment, and the more options available at our disposal, the better the healthcare outcomes will be. I’ve always thought of EoE as a disease of literal blockage, and with acupuncture, treatment is all about removing those blockages, so this makes perfect sense. I certainly benefited from acupuncture treatments, and it improved my stress as well, which subsequently improved my EoE. It’s all connected!
Hello Juston,
Thanks for your article ! Much more refined an approach than the mainstream.
Just about cow milk and wheat in regular chocolate and beer: did you consequently stop having them ?…
Kind regards from Geneva, Switzerland
Gideon
Response from Juston: “I stopped consuming cow’s milk and wheat entirely for several months. Thankfully, I was able to obtain dark chocolate (one of my favorite foods) through a variety of companies that don’t include milk in the ingredients. With respect to beer, I noticed that alcohol tended to exacerbate my symptoms, so I significantly cut back on my EtOH consumption. There are many gluten-free beer products on the market today which also make it more feasible. I do think alcohols removal during the healing process is required for optimal results and to drive down eosinophilic predominant infiltration in the GI tract. When in doubt, less is more.”
Hello again, I wondered why the article does not include any reference to Seema ACEVES’s work, one of the EoE-pioneers, in San Diego.
Thank you,
Gideon
Hello my daughter Maya is 12 years old and was diagnosed with EOE at the age of 8. Maya is currently on Flovent and her symptoms have worsened over the past several months. She had a scope in July and her eosinophil count has increased significantly compared to her prior scope. We increased her Flovent dose last week. We have tried different holistic approaches in the past that didn’t seem to make difference. If we can find something that can naturally improve her disease I am all in. Are you seeing patients?
Hello Rebecca, please reach out to our clinic (203)304-9502.
So if all those food groups need to be removed, what am I supposed to eat? Any guidance would be super helpful thanks!
Hello Stacy, it’s best to work with a nutritionist to guide you, especially if you aren’t sure what to eat instead. Our team is well versed in guiding patients through this journey.