How He Reversed MS & Beat a Stroke | Montel Williams
Listen to Episode 46
Summary (full transcript below)
Endotoxemia. A fundamental driver of chronic disease. What is it? And more importantly, what do we do to address it? In my podcast with Dr. Jill Carnahan this month, she unleashes a torrent of compelling science and clinical savvy on all things endotoxemia. From heart disease and diabetes to autoimmunity (genetic or acquired) and mast cell activation, Dr. Carnahan is clear that pathological intestinal permeability (she discusses testing, but at this point in her career believes most everyone who sees her with chronic disease has IP) drives inflammation by allowing excess microbial endotoxins- primarily as lipopolysaccharide (LPS) – to enter circulation. Focused on root cause functional medicine (toxins, diet, infection, genetics), she concurrently heals the gut to drop the inflammatory burden. A key intervention for Jill is sugar-free, GMO-free, serum-derived bovine immunoglobulin (SBI), and we spend quite a bit of time on why SBI is crucial. With 43 human trials behind it, if you are not using SBI yet, you’ll be compelled to start, I suspect. We also have a fun dialogue on the role of fatty acids and toll-like receptor activation, connected directly to LPS. Jill shares a handful of very compelling case vignettes AND talks candidly about how she set up an extremely successful functional medicine practice and positioned herself as an expert in the field. And let me know: will you be changing how you prescribe high-fat diets based on the research we discuss?
In functional medicine, all roads lead back to the gut—and that is where pioneering functional medicine practitioner Dr. Jill Carnahan focuses her attention when working with patients to ease and heal chronic conditions. Board certified in both Family Medicine and Integrative Holistic Medicine, Dr. Carnahan uses a multipronged approach to healing the gut—including stopping lipopolysaccharide production in the bloodstream, tightening the loose junctions of the gut, and increasing mucin production—to help patients realize amazing results. In today’s conversation with Dr. Fitzgerald, Dr. Carnahan walks through her favorite strategies for healing the gut, treating root causes of disease, and easing symptoms. She also offers advice to practitioners who want to open their own functional medicine practice.
In this podcast, you’ll hear:
- What endotoxemia is and how it needs to be addressed as a Root Cause of illness
- How zonulin increases lipopolysaccharides in the bloodstream
- Tests for endotoxemia (and why Dr. Jill only uses one or two of them)
- When a high-fat diet is appropriate for a patient—and when it’s not
- The effect of environmental toxins on the microbiome
- The importance of increasing mucin production in the gut (and not just healing the loose junctions of the gut)
- The benefits of using serum-derived bovine immunoglobulins (SBIs) to heal the gut
- How SBIs are preferable to colostrum and glutathione
- SBI use for SIBO and SBI use in very young children
- Dosing and duration of SBI intervention for a variety of conditions
- How some supplements on the market unintentionally make mast cell conditions worse
- Diagnosing tick-borne illnesses
- Advice on launching your own functional medicine practice
Dr. Jill Carnahan
Dr. Carnahan completed her residency at the University of Illinois Program in Family Medicine at Methodist Medical Center. In 2006 she was voted by faculty to receive the Resident Teacher of the Year award and elected to Central Illinois 40 Leaders Under 40. She received her medical degree from Loyola University Stritch School of Medicine in Chicago and her Bachelor of Science degree in Bio-Engineering at the University of Illinois in Champaign-Urbana. She is dually board-certified in Family Medicine (ABFM) and Integrative Holistic Medicine (ABIHM).
Dr. Jill was also part of the first 100+ health-care practitioners to be certified in Functional Medicine through the Institute of Functional Medicine (IFMCP). Following residency, Dr. Carnahan’s vision for health and healing resulted in the creation of Methodist Center for Integrative Medicine in Peoria, IL where she served as the Medical Director for 4 years. In 2010, she founded Flatiron Functional Medicine in Boulder, Colorado where she has a widely sought-after medical clinic with a broad range of service including medical and nutritional consultations, and massage therapy.
Dr. Jill is a 17-year survivor of breast cancer and Crohn’s disease and passionate about teaching patients how to “live well” and thrive in the midst of complex and chronic illness. She is also committed to teaching other physicians how to address the underlying cause of illness rather than just treating symptoms through the principles of functional medicine. She is a prolific writer, speaker, and loves to infuse others with her passion for health and healing! Visit www.jillcarnahan.com to learn more.
Podcast Sponsor – Ortho Molecular

Why Choose Ortho Molecular Products?
There are many choices in the dietary supplement market — an overwhelming number of companies selling a dizzying array of products, all promising results. As a healthcare practitioner making recommendations to your patients, you feel a responsibility to sort through those options and find the best products to support the health of those who have put their trust in you.
Shownotes
Full Transcript
Dr. Kara Fitzgerald: Hi everybody. Welcome to New Frontiers in Functional Medicine where we are interviewing the best minds in Functional Medicine, and today is definitely no exception. I am thrilled, thrilled, thrilled to be talking to Dr. Jill Carnahan. She’s a treasure, a thought leader in Functional Medicine and we will be covering just a whole bunch of information I think you’re going to find will influence your practice.
Let me give you her background. Dr. Carnahan completed her residency at the University of Illinois, Program and Family Medicine at Methodist Medical Center. In 2006, she was voted by faculty to receive the resident teacher of the year award and elected to central Illinois 40 Leaders Under 40. I’m not surprised. She received her Medical degree from Loyola University Stritch School of Medicine in Chicago, and her Bachelor of Science in Bioengineering at University of Illinois in Champaign Urbana. She’s duly board certified in both Family Medicine and Integrative Holistic Medicine. She was one of the first group to receive her Functional Medicine certification through IFM, and in fact, we’re going to be talking today about a really lovely presentation she gave to the — this year, the 2018 — Annual International Conference in Florida, so we’ll be hopping into that in a second.
Following her residency, Dr. Carnahan’s vision for health and healing resulted in the creation of Methodist Center for Integrative Medicine in Peoria, Illinois, and she was the Medical Director there for four years. She founded Flatiron Functional Medicine Center in Boulder, Colorado, in 2010. It’s just been a really great, extremely successful clinic ever since, and I hear good things coming out of Flatiron all the time. Jill, welcome to New Frontiers.
Dr. Jill Carnahan: Thank you, Kara. I love talking to you, because we love to dig into the science, and it’s always just a joy to find such a kindred spirit, so I’m excited about our topic today.
Dr. Kara Fitzgerald: Yeah, absolutely, and you’ve been really kind of an inspiration for me how you’ve launched your practice. Not only are you a good (practitioner), you go into the rabbit hole I think as much as I do with regard to really looking at and metabolizing the science and then applying it in practice. But you also have built this wonderfully successful functional medicine clinic, and I want to circle back and pick your brain on that a little bit at the end. I want to devote just a minute or two, because a lot of people listening to New Frontiers are clinicians transitioning into functional medicine, and it’s that deer in the headlights moment, and you’ve done it. You’ve been there for years, and you’ve built this lovely successful thing, so let’s make sure we circle back.
Dr. Jill Carnahan: I would love that. You got it.
Dr. Kara Fitzgerald: We’re going to talk about all things endotoxemia and what to do about it. It’s been something that those of us in the functional medicine space have been talking about for years, but give me the background. What is endotoxemia?
Dr. Jill Carnahan: You asked a great question: What is endotoxemia? What we find is this is at the root cause of so many chronic conditions from obesity, diabetes, cardiovascular disease, depression, anxiety, even chronic pain and autoimmune disease. As we like to think with functional medicine we’re going to the root cause, well this is the root cause of so many things that we see every day in clinical practice.
What we see is basically many, many of our patients, in fact — I don’t know about you, but — at this point I usually just assume that my patients have leaky gut or intestinal hyperpermeability, and when these tight junctions are disrupted from environmental toxin or infection, and the zonulin is increased, there can be a crossover of the bacterial polysaccharides which is called LPS, lipopolysaccharide, from the intestinal lumen into the bloodstream. And when it gets in the bloodstream, the body sees it as a bad guy, and an antigen, and it’s a potent, probably one of the most potent immune stimulators that we know of. This stimulates the immune system, causes chronic inflammation, all of these inflammatory cytokine processes because it’s not supposed to be in the bloodstream. And that’s really at the core what endotoxemia is, is this LPS bacterial coating crossing over, triggering an immune response in the bloodstream.
Dr. Kara Fitzgerald: And leaky gut is the fundamental driver of this translocated LPS.
Dr. Jill Carnahan: Exactly.
Dr. Kara Fitzgerald: That’s amazing.
Dr. Jill Carnahan: You have to have some sort of permeability, but obviously we have so many people with a permeable membrane, and these are not like bad, horrible pathogens like giardia or cryptosporidia; these are coatings of some of our normal residents in the gut. What happens is pretty much anybody with significant intestinal permeability can have some degree of endotoxemia.
Dr. Kara Fitzgerald: Talk to me about how you’re addressing this clinically. You must be thinking, you’re going to be addressing intestinal permeability and treating that, but you’re also going to be thinking about diet, lifestyle modification, and removing the mediators of intestinal permeability. All your patients you are assuming have some degree of endotoxemia, because everybody’s coming to you with leaky gut. And you did just give me a list of conditions, and it goes on from there. What are you thinking about in terms of addressing it?
Dr. Jill Carnahan: Yes, again, there are tests out there that you can do. Cyrex Array 2, there’s the old mannitol/lactulose test. Honestly, I do not even test any longer. I do sometimes do food sensitivities, and when I see tons of antigens and autoimmunity, I just assume it’s there.
Dr. Kara Fitzgerald: Yes.
Dr. Jill Carnahan: I would say the types of patient we see we can just assume that must be part of the problem. I think it’s partially because of, I always think of nowadays with my complex patients it’s all about infection and toxin and which piece is bigger. It’s like a seesaw. We know infections like viruses and bacterial pathogens and SIBO, and SIFO, and parasites can all increase the intestinal permeability. So can food antigens like gluten and other inflammatory things in the diet, and then things like environmental toxic exposure, so chemicals, pesticides can cause this, and also mold can cause this. So there’s so many environmental triggers like infections and toxins that our patients are exposed to, and they are increasing intestinal permeability.
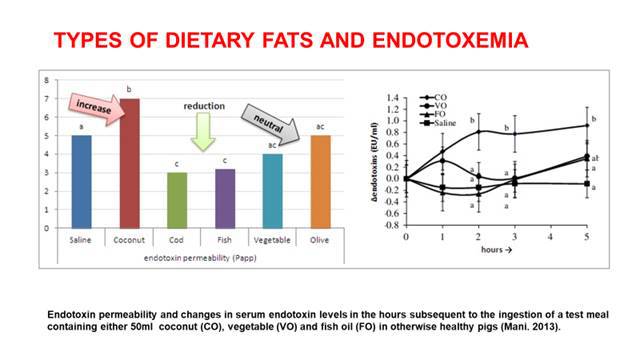
It’s funny, because we’re all doing these Paleo-keto diets. I’m a huge fan. I use these in clinical practice all the time, but there is clear evidence that fats in the diet, especially coconut and saturated fats increase endotoxemia, so I think there’s a subset of population where, say we have someone with a previous heart attack. We may not want to put them on high saturated fat, because we’re going to increase that risk of endotoxemia.
Dr. Kara Fitzgerald: That’s a pretty profound statement. I use a high-fat ketogenic diet in practice, too. Yes. I think it’s incredibly interesting, and I think it’s worth actually drilling down. I think we need to … I’m interested in seeing data, and especially human data, where it’s actually measured, you know, baseline and follow-up.
Dr. Jill Carnahan: Yeah, there was a study in 2013 that was just actually republished in the fall of I think 2017 where it actually showed the types of saturated fats in the LPS serum levels, and what it showed was coconut showed increase, olive oil was neutral, saline was neutral, and then cod and fish oil EPA, DHA, was all reduction. This blows my mind, because I’m like you; I really use and prescribe ketogenic and Paleo diets in my practice frequently, so I use these all the time, and just to be clear, I am still a fan of all those.
Dr. Kara Fitzgerald: Yes.
Dr. Jill Carnahan: But I think you have to understand the process when you are giving patients high saturated fat, because there’s a certain subset on the diabetic, obese, person who’s had a heart attack, that probably wouldn’t do great until you heal their gut.
Dr. Kara Fitzgerald: Let me give you my thought on this. I think you’re right, and a piece of it has to do with the milieu that you’re introducing it into. This is an argument for treating gut first without question. But I’m wondering; in the study they introduced it with a diet that’s rich in carbohydrates, so my question and what I’d really like to see answered is if you introduce these fats without the carbohydrate macronutrient accompanying them, would they behave differently? Would the cascade of hormones being released, because if it’s a carbohydrate meal, obviously insulin’s going to be there, whereas if you introduce high fats in a keto meal, insulin is not going to be introduced, would that have a different outcome? That’s one of the questions I’m sitting with. It would argue for a potential anti-inflammatory effect in the keto diet, but it might not. I could be wrong here, but it’s a question that I have, and it’s an argument for potentially managing how we introduce macromolecules or food combining.
You don’t want to eat potentially a high fat saturated meal or use coconut oil or medium chain triglycerides which are extremely popular when you’re having a sandwich or an ice cream. Does that make sense to you?
Dr. Jill Carnahan: Yes. I completely think there’s a key to that, too. And I’ll just tell you a story, because it shows a significant, so I had a patient who — here’s what happened; what in the world do you think happened? And she said okay, I can eat eggs and I eat coconut oil all the time and never had trouble. But the other day I cooked the egg in coconut oil, and I had the most severe allergic reaction of my life. And I had to think about that, and I thought okay, she’s got a little bit of sensitivity, maybe even IgE to eggs. She didn’t know whether it was maybe small quantities. She threw that in the coconut oil and it drove it right transmembrane just like endotoxemia, the antigen. I really believe it was because the driver of the coconut oil really does increase endotoxemia. And it blows my mind, but that was such a clear example, that I don’t know for sure, but that’s my theory on what happened.
Dr. Kara Fitzgerald: Yeah, right. Which would argue against my idea that the introduction of sugar drives the endotoxemic effect of these fatty acids — of some of the fatty acids, because as you pointed out, olive, fish, those oils, were actually either protective or reduced. I think there’s more to know. [crosstalk 00:11:57] Yeah, go ahead?
Dr. Jill Carnahan: I do. And I agree with you. It’s like, oh, I love the high fat diets. I think they’re incredible for patients with all different types of various conditions, especially autoimmunity. But then I’m like okay, we just have to be a little cautious, because-
Dr. Kara Fitzgerald: Yes.
Dr. Jill Carnahan: … there may be more than we really understand. I still prescribe them, and I do it myself, but I think that there’s more understanding to be had, because fascinates me like why would that be the case, and it is in the research.
Dr. Kara Fitzgerald: Yes. I think your thought around healing a gut, starting with the gut, is well taken by me. I think that’s an important idea. It’s just like, let me throw out one more, and then we can kind of back up and move on, but this is such an important topic. You know the other piece is that in a very oxidative environment, i.e., in somebody who’s got uncontrolled Type 2 diabetes, you want to be mindful about introducing omega-3 fatty acids immediately, because they’re polyunsaturated and you can increase oxidative stress with those polyunsaturated molecules. Or you want to introduce the fish oil, because it’s so remarkably helpful with a good anti-oxidant as well. I hear what you’re saying, Jill, and you make really interesting and important points. I think it’s particularly important at this time that we push this conversation forward while we’re also actively prescribing higher fat diets. And many of us are leaning on medium chain triglycerides as well. Are we introducing them into a safe environment?
Dr. Jill Carnahan: Yeah. Completely agree. And again, I use it, too, so it’s just a query that we need to … you and I like to ask these questions we’re hearing.
Dr. Kara Fitzgerald: Yep, absolutely. All right. What are you doing … you’ve talked about toxins and you put the Standard American Diet strongly into the toxin column. And then you’ve talked about infection. Any comments around lifestyle modification, and then I want to talk about some of the nutraceutical interventions that you might be doing for this.
Dr. Jill Carnahan: So there’s definitely the pesticide chemicals, things like that so glyphosate in our diet and in our food supply and even chemicals and plastic and things, and so I think the first place we start is always diet. What I do to help leaky gut with diet is first of all check for food sensitivities. These would be the IgGs that are very highly elevated, because those are going to also increase inflammation, and you take those foods that we, for 15 years now, have both prescribed elimination diets, and I use that as a core, because those foods, especially gluten, are going to be a big trigger as well. So you decrease the antigenic load. That’s number one.
And then number two is organic is absolutely essential nowadays, and many of our patients can’t afford all organic, so at least the dirty dozen from environmental working group we can avoid those if possible at all costs or eat organic. And then non-GMO is big because glyphosate has a huge effect on the microbiome. In fact, the studies said, “Oh these…Monsanto said they don’t hurt human cells; all is good.” But the problem is they dramatically alter the microbiome. It’s been shown to preferentially kill lactobacillus and allow clostridia to overgrow, and we all know that’s a big problem.
Getting rid of the glyphosate by eating non-GMO foods is also really critical. Just a clean, whole food diet, lots of fruits and vegetables, leafy greens, nuts and seeds. I think kind of a Mediterranean with a little bit lower carb is kind of where I lean with healing a leaky gut and then taking out the gluten, the dairy, the sugar, and the other foods that are sensitive.
Dr. Kara Fitzgerald: Perfect. That’s perfect. By the way, folks, in the show notes I’ll list the dietary fats in the endotoxemia paper that Dr. Carnahan just referenced, and Jill, if you can send me that last, that would be great. And we’ll just make sure those are posted in the show notes so that you can access those studies. What about nutraceuticals? Are you thinking about those in regard to addressing endotoxemia and leaky gut?
Dr. Jill Carnahan: Yes, 100%. There’s so many different ways where this … like if we can neutralize the lipopolysaccharide, that’s like at the core source. That’s one way we can do this. We can increase mucin production at the cellular level and actually increase the protective coating; that’s another. If we could increase tight junction expression and decrease the actual permeability, that’s another. And then just really healing the gut. I think about it in several ways. The old school glutamine is still okay. I feel like the power isn’t there as much as some of the newer things we can do.
The new kid on the block that I love is serum-derived bovine immunoglobulins. Now, these are where you actually neutralize the LPS. These are passive immunoglobulins that go around and grab those particles of LPS and actually prevent it from transferring over into the immune system.
Dr. Kara Fitzgerald: That’s wonderful actually. There’s a lot of good data out on SBI or serum derived bovine immunoglobulin. Just talk to me about some of it.
Dr. Jill Carnahan: Some of the research behind … first of all, they’ve been generally recognized as safe for a decade, so since at least 2008. There’s over 43 human studies and 6 randomized placebo controlled trials, so there’s lots of evidence that this is not only safe, but effective. The one that I use, which is an over-the-counter serum derived bovine immunoglobulin is dairy free, sugar free, non-GMO, which as we just talked about is a pretty critical thing. There is a prescription grade one on the market that has GMO corn dextrose, and so obviously for reasons we just discussed, I could really not see using. It’s from USDA certified, clean, medical grade cattle, and it’s isolated from the colostrum of the cattle. In my mind, it’s similar to … I think it’s way better than our old products like colostrum but it has the same idea of this passive immunity that would give any-
Dr. Kara Fitzgerald: Why do you think it’s better than colostrum, just out of curiosity?
Dr. Jill Carnahan: Yeah. You got it. I have about 50% of my patients that react to egg and dairy, and all the previous products on the market had egg or dairy, and they had reactions to them. This one I still, I don’t think I’ve had one patient that had a reaction to it, which is nice.
Dr. Kara Fitzgerald: Oh, that is. That’s great. Okay, so keep going with the background on it.
Dr. Jill Carnahan: This has been used and just well-studied, so it’s very safe. I use it in as young as two years old, so very, very safe product. It’s a powered form, you can mix it with water or some other liquid. You could put it in a smoothie. I think it tends to work better between meals or before a meal, but in cases of compliance, then you can even mix it with food or a smoothie. It gives passive immunity. So again, it actually has really good research on binding some of these bacteria coatings. I think it shows lipopolysaccharide, C. diff toxin A and B, some of the different particles of the microbial components. It actually shows studies on binding H. pylori, listeria in mycoplasma. And even there’s studies on binding viruses and viral analog, so this is a pretty cool way to give passive immunity.
Some of the things that I think about, like obviously we talked about endotoxemia in most of our patients, but one of the things that’s a big thing for me is seeing a low fecal IgA, like a secretory IgA that’s low. You see those a lot, too. And basically, that tells me the mucosal immune system is just trashed. I love this product for low sIgA, because I think about giving them a passive immune system is going to help with getting rid of the pathogens and the overgrowths and all those things.
Dr. Kara Fitzgerald: You know, it also apparently binds zymosan pretty effectively. You’d think about this in…
Dr. Jill Carnahan: Yeah.
Dr. Kara Fitzgerald: … do you think about it in your SIFO patients or do you think about it in your yeast patients and do you use it in SIBO, out of curiosity?
Dr. Jill Carnahan: I do. 100% in both of those cases, because what happens, you know yeast is opportunistic, so I always tell patients you know what? Your root cause is a weakened immune system. You don’t get a huge overgrowth of yeast unless you have a weakened system. And so because of that, I understand that anytime we can support … like I love going to the root cause and just throwing antibiotics or antifungals at them may be temporarily a good idea, but my job is what’s really causing this. And so many times it’s their weakened immune system, their low sIgA, and this in my mind is about as close as we can get to IVIg. It’s a product that will actually aid their immune system in fighting pathogens.
Dr. Kara Fitzgerald: That’s amazing. So, in somebody who’s got a very active autoimmune process going on where you might consider IVIg, you’re thinking about you’re actually going to use SBI at this point, oral SBI.
Dr. Jill Carnahan: I do. And you know, the approval for insurance and the expense, I mean, that could be $8000 to $10,000 a pop and they get it every two to three weeks, so it’s incredibly expensive. Insurance may or may not cover it. But if I have either a low serum sIgA, which is actually a secretory IgA deficiency syndrome, or a fecal sIgA low, both of those conditions I’m thinking their mucosal immunity is weakened; what can I do that’s easy, affordable, and this is the first thing I do every time.
Dr. Kara Fitzgerald: That’s awesome. It’s really a useful pearl. How are you dosing it?
Dr. Jill Carnahan: The studies have all used 5 grams twice a day, which is two scoops twice a day of the over-the-counter product. And some patients who are just maintenance, I’ll do one scoop twice a day. But somewhere between one and two scoops twice a day; pretty simple dosing, too.
Dr. Kara Fitzgerald: Wow. Okay, so you’re sticking with that two scoops in the patients with higher need? You’re not going higher than that?
Dr. Jill Carnahan: Some situations where it had like an active Crohn’s or colitis, I’ve used up to eight scoops, and especially for acute diarrhea where nothing else works, it tends to work really nicely at the higher doses, so I’ll use it in those cases at higher doses up to four to eight scoops a day. But I haven’t in general gone a lot higher for the average patient.
Dr. Kara Fitzgerald: What’s the duration? What duration are you using it in your chronic folks?
Dr. Jill Carnahan: I would say minimum of six months. And I have to tell you another story. This is just from last week. I had a patient who I saw two or three months ago, and she actually fit the criteria for combined variable immune deficiency where she had low serum total IgG, and then she had some other markers that just showed she was having chronic sinus infections and respiratory issues. So I referred her to my local immunologist who I work with, and I said, “You know what? She’s a candidate for IVIg. She’s got combined variable immune deficiency.” So he saw her, did a bunch of labs and workup, and the time between me seeing her and getting a plan in place and her seeing the immunologist was about four weeks. And what he prescribed was a micellized mushroom and I prescribed SBI, so two things that would increase immunity and hopefully increase … so I don’t know which one helped, but here’s what happened.
She went back to her follow-up visit with the immunologist, and he said “I don’t know what you did, but your immunoglobulins are totally normal and you no longer have an immune deficiency.
Dr. Kara Fitzgerald: Wow.
Dr. Jill Carnahan: And I was blown away, because she on her first visit said, “Well, I’m seeing Dr. Jill and she gave me some oral stuff,” and he immediately was like “oral stuff doesn’t work.” Like he just blew her off. And then she comes back and he’s like blown away. He’s like “I don’t know what you did.” And one of the two interventions was SBI … it was just serum bovine immunoglobulins, and it was just profound of how impactful it was.
Dr. Kara Fitzgerald: That’s incredible. And how was she clinically?
Dr. Jill Carnahan: Much, much better. Like she had respiratory…
Dr. Kara Fitzgerald: Yeah, go ahead.
Dr. Jill Carnahan: … well of course she had chronic respiratory things, and I treated locally with a nasal spray, but when we repeated the labs, the immunoglobulins were normal. I’ve never seen…
Dr. Kara Fitzgerald: That’s incredible.
Dr. Jill Carnahan: … it really was powerful.
Dr. Kara Fitzgerald: That’s really, really exciting. Let me ask you in general. For this patient, I’m assuming you were using the chronic protocol, which is one scoop twice a day?
Dr. Jill Carnahan: It was two scoops twice a day for her.
Dr. Kara Fitzgerald: Two scoops twice a day, okay. Really impressive. Thanks for that, Dr. Carnahan. Now, what about other labs? You talked about in the beginning that you might look at food sensitivities, the Cyrex Array 2 you used to use, but you assume everybody has leaky gut, and I’m with you on that. I think any of our chronic patients we can really assume that, especially if they’ve got food reactions and they’ve been on a Standard American Diet to any extent. What about inflammatory markers? Are there any … oh, well you’re looking at IgA, you’re looking at secretory IgA or you’re measuring serum IgA. Are you looking at CRP or sed rate, or oxidant stress markers, or any of those that you’re seeing favorable change with when you use SBI?
Dr. Jill Carnahan: When I think about leaky gut, and if I’m just doing serum labs, because like we said, typically I don’t do a specific leaky gut panel, what I’m doing, I do total IgG, and I do subtypes of IgG, and then I’ll do IgM, IgA, IgE. I’ll do all the immunoglobulin levels. I also do MSH frequently because a really low MSH is classically associated with an increased intestinal permeability.
Dr. Kara Fitzgerald: And that’s melanocyte stimulating hormone, folks.
Dr. Jill Carnahan: Correct. And there’s obviously connections to all kinds of things, but definitely mold exposure can be a cause of low MSH, and almost always … I had some studies on mycotoxins in children in Africa, and there was a clear association with massive increase in intestinal permeability, and it was related to the low MSH. And they did in those studies, they used vitamin A, vitamin D, zinc, zinc carnosine. They didn’t have anything like serum derived bovine immunoglobulins, or I think that would’ve helped, but they did those things for that permeability and improved a little bit. So I’ll check the MSH and then I’ll check kind of infectious burden, so I’ll often check viral titers in mycoplasma, chlamydia, check for tick-borne stuff, so just checking those kinds of things. I’ll usually do a urine screen for both toxic exposures and also molds. I’m looking at both toxin and infection and triggers in the more complex patients.
Dr. Kara Fitzgerald: Okay, good. All right. A comprehensive workup. Just out of curiosity, what are you doing for your tick-borne? I know that people are going to have questions. Actually, they’re going to want to know your whole protocol and all the labs that you’re doing, but just, we can simplify it and think about tick-borne. What lab are you using or labs?
Dr. Jill Carnahan: I still love IGeneX. It’s kind of one of the old really great ones. I also use DNA Connexions, which is a urine PCR for tick-borne illnesses and co-infections. And there’s a couple, there’s ArminLabs from Germany and some difficult patients and Galaxy for Bartonella.
Dr. Kara Fitzgerald: Okay, perfect. Thanks for that.
Dr. Jill Carnahan: You got it.
Dr. Kara Fitzgerald: All right. Clearly just as judging by the patient you just presented, you’re seeing your followup testing is coming back improved, but I suppose where the rubber meets the road is clinically you’re just seeing really nice outcome.
Dr. Jill Carnahan: Yes. Yeah, I see people. Normally the only thing I guess this would be the same like if you use a binder. This is not a binder, but it does bind toxins in a passive immunity way. And I think the one risk is someone with severe constipation. People with really bad constipation are the only class that I find I have to be a little more cautious and starting slowly and working up. So if you have some severe, I would treat the constipation first, and then start slowly, like maybe one scoop, one half scoop, and work up to two or three or four scoops a day on a patient with severe constipation. But again, in my mind there’s a root cause, so you actually fix the constipation first and then there’s no problem, because it’s not contraindicated; it’s just that you want to be cautious.
With looser stools, patients love it, because they tend to be a little bit more regular. And labs, yeah, the follow-up; it’s always depending on the root cause, so if there really is a tick-borne infection or a toxic exposure, the SBI will help them, but it won’t solve the root cause, so I still go back to whatever the root is causing that issue. But it’s an amazing Band-Aid in the meantime that really, really helps the patients clinically.
Dr. Kara Fitzgerald: Right. It’s just repairing some of the damage, as we’ve talked about, and, however, you’re still concurrently doing a full functional approach.
Dr. Jill Carnahan: Yes.
Dr. Kara Fitzgerald: That’s really nice. I’m assuming that this is, well this is clearly going to be your first go to before you refer to IVIg, but you really think that this might supplant it?
Dr. Jill Carnahan: Not really, because the people who truly have a combined variable immune deficiency, they’re not going to resolve; I mean, that was so unique, that case, and so I don’t know if there was something else driving it. But here’s the thing: I don’t have this all figured out, but what I do see is there’s a degree of patients with extreme and basically protein wasting enteropathy. This is a diagnosis which means they’re basically wasting protein, losing it through the permeable gut. And so, if you’re losing your immunoglobulins and proteins through the permeability of the gut and wasting them, getting back some immunoglobulin and actually healing that leaky gut may improve that immunoglobulin level.
And I find my subsets of IVIg requiring patients definitely usually have an infectious or a toxic burden in the lungs or the gut that’s driving that. There’s a subset that are genetic, and then those you probably aren’t going to change. But I think it’s interesting, because I think in the small subset it actually could be either an adjuvant or a cure for those … I hate to say the word cure, but at least improvement in their state.
Dr. Kara Fitzgerald: Yes, that’s really impressive. Well, and even in the people with genetic, they’re still going to have environmental influences that may actually be greater than the genetic influence.
Dr. Jill Carnahan: Yeah. And, you know, I want to just mention something that your listeners may not think of, other things that might be helpful. Of course like Crohn’s or colitis, you’re going to have a permeability, so I would definitely use this product in patients with Crohn’s or colitis. We mentioned autoimmunity, so almost any autoimmune case there’s going to be a permeable gut. Lyme and mold, of course, are big toxic infectious burdens. Autistic children, this is great, because they often have really tough guts. And then two we may not think of that we probably don’t see super often is post chemotherapy and HIV.
Dr. Kara Fitzgerald: Yes. Right.
Dr. Jill Carnahan: Because those are two really great situations where you can use this, too.
Dr. Kara Fitzgerald: That’s perfect. Well, listen, I think that I just want to pick your brain as I’ve been doing on this topic. Well, actually, let me ask you one more question. I want to get your thinking just with regard to being a thought leader in our space and just talk to you a little bit about how you would advise clinicians coming into the field. But you’re also a mast cell expert, and I think that you use SBI in your allergic/mast cell activation folks. Any comments on there, or any little case vignettes you can offer?
Dr. Jill Canrahan: I do. And that would kind of go back to the previous products in the market always cause sensitivity, like no one could take them, because the prescription brand had dextrose, which if you have SIBO or SIFO, you’re going to feel miserable if you take a product with sugar in it. It’s just like crazy to me, and not only that, but you’re getting a corn source that’s not non-GMO. It’s GMO corn. So there are some big issues, red flags for me. And then the previous products that were out there had either dairy or egg, and really most of my patients with the mast cell stuff, those were massive triggers, so they could never take this product. Now they can. So I do like it for that reason.
Dr. Kara Fitzgerald: Yes. That’s really terrific. Okay, so talk to me about your starting points for new functional medicine clinicians coming into the field and hanging out their own shingle and finding their community. What are some of the things that you did that you’re continuing to do?
Dr. Jill Carnahan: Yeah, great question, because it’s funny, you think back, and we all start somewhere, and I know when I started I really didn’t know anything of what I was doing. But a couple of things I feel guided me. First of all, I was passionate about functional medicine. I was so like there was nothing else I could’ve done. And I think most of the practitioners that are starting into it feel that virus where they get infected and we can’t not talk about it or not study about it. I’m a lifelong learner like you, so I’m constantly reading, studying, and trying to know the cutting edge of what’s out there.
But as far as what I did, I started just talking to community groups. I went to the local Life Time Fitness and gave lectures, and really just met other practitioners. And I’m of the mindset — I’m sure you’re the same, but — there’s more than enough business to go around. So I could have a doc that literally opens his clinic two door down from me, and I’ll invite him over for coffee and say, “How can I help you?” Like really helping and loving other practitioners is so key, because we all need each other, and it’s not a competitive world. There’s just so much business to go around.
Getting to know people that, whether it’s acupuncture, massage therapy, other therapies, or even other doctors, and then really trying to help them any way that you can or even partner with them. And start small. I remember coming from … I came from a big medical center in Troy, Illinois, where I was Medical Director. I had a multimillion dollar clinic with seven exam rooms, procedure rooms, two RNs, I mean, I had so much overhead, it was crazy. Loved it. It was beautiful.
But when I started in Colorado, I shared space with Bob Roundtree, and we started with one shared exam room with one person answering the phone, like so simple. But it helped me, because I had no debt. I started very small, I grew into my practice, and all the way I just slowly, slowly got more space, got more … and so starting with low overhead is really important, because if you get in over your head, then you become a slave to your clinic, and then you’re back in the same position where you left.
Really starting low and small and then getting the word out. And you need an online presence nowadays. I hate social media, but I need it and I use it frequently, because that’s the way to reach and make an impact. Whether you do it yourself like I did for eight years, writing content and getting that out there, but you need a good web presence, you need a good social media team or yourself in the beginning. And that’s really going to drive people to you as they search online. And nowadays that’s the biggest source of referrals.
Dr. Kara Fitzgerald: Would you say that that is what kind of transformed your practice from the simple setting that you started out in to where you are now, where, I believe you’re booked out for a year or so.
Dr. Jill Carnahan: We have a 5-year waiting list, and we’re not taking new patients, so it’s pretty crazy.
Dr. Kara Fitzgerald: It’s huge. Wow.
Dr. Jill Carnahan: But yes. What was your question about how it changed since starting?
Dr. Kara Fitzgerald: What was the biggest influence in getting, basically shutting your practice down because you’re so booked out? What would you say the piece was that really pushed that forward?
Dr. Jill Carnahan: Eight years ago, I decided, okay, I need to kind of figure out who I am. And I actually branded Dr. Jill, your Functional Medicine Expert as a registered trademark. And I really was like okay, but what do I want to do? I wanted to be the expert. And so I named myself the expert. I stood up to learning and studying so that I could be the expert, but I actually branded that and became what I wanted to be, and it manifested. It’s kind of profound to me of how that happened.
I really do feel like I am an expert now, but at the time I branded myself, I wasn’t. And I just grew into that, and how I grew into it was I backed it up by writing articles. I wrote an article every month. Now I have some help, but for the longest time I wrote everything myself, and I just put out what I thought was really good content on stuff that I was interested in. And so that started helping the reputation, because people would search for mast cell disorders and they would find my article, or mold illness, and they would find my article. That driving the writing and the content is what’s going to drive your presence, and the online presence is really going to drive your people who want to see you in the clinic.
Dr. Kara Fitzgerald: You’ve done a really lovely job. I just want to underscore the fact that you said you wrote about what you love, and that’s essential. Actually, you identified what you love. So a few things you said: One, you created yourself as an expert and now you’ve grown into that fully, which you absolutely have. And you defined what you were going to be expert in and what you had the most energy around. And then you created the vision and it happened. Incidentally, this idea of there being abundance and no competition, you’ve supported me. Actually, I’ve picked your brain on multiple occasions regarding your fabulous clinical business model. And I know we’ve co-supported each other, but…
Dr. Jill Carnahan: You’ve supported me to other things. You’ve done the same for me, too. I want people to know that,
Dr. Kara Fitzgerald: It’s a really lovely relationship, and I am of the same mind, that abundance happens, and if we allow it to happen if we get out of the way of the abundance happening.
Dr. Jill Carnahan: Yes.
Dr. Kara Fitzgerald: Thank you so much for your time today, Dr. Carnahan. You’re just a real treasure, and without question, you’ve influenced the folks listening and I know people are excited about SBI. Thank you for everything you’ve presented here today.
Dr. Jill Carnahan: You’re welcome. It was fun. Thanks so much.
Dr. Kara Fitzgerald: Great.
Related posts






Do you know the SBI Jill uses that she discusses?
Yes, it is Orthomolecular SBI Protect
Please advise as to the brand of SBI Dr. Carnahan was referencing in this podcast. Great info! Thank you!
Orthomolecular SBI Protect — you’re welcome!
Is the brand name or manufacturer of the SBI Dr. Carnahan uses ever mentioned? I’d really love to know the exact product being referred to here.
Orthomolecular SBI Protect
Great interview with Dr. Carnahan, are people recommending SBI protect be taken with food or on an empty stomach?
Really enjoyed this conversation. I am newly practicing FxMd. May I know the name of the OTC SBI brand? Many thanks.
I’m so glad! IT is Orthomolecular SBI Protect
What is the name of the SBI being used? I’d love to be able to try it.
Orthomolecular SBI Protect
Great info, thanks! Have you ever used SBI Protect in someone who is sensitive to beef protein?
Initially it’s best to avoid using SBI in a patient with IgG until intestinal permeability is improved. As gut barrier function is repaired, tolerance to beef should improve. Begin with a careful challenge, starting slowly and gradually increasing to therapeutic dose.
thank you very much for sharing this podcast. Are you able to mention which mushroom product was used that was referenced in this discussion?
We’re currently using JHS mushroom supplements as well as Jeff Chilton’s line Nammex and finding good results.
Dear Dr. Kara, I started taking the SBI Protect powder a week ago, only 1 scoop/day so far, and I experience Strong nausea and headache. Is it normal to have these symptoms? Thank you!
I’m sorry to hear that, Heni. We use it a lot in our practice and it’s generally well-tolerated. I would suggest dialing back the dose until you are symptom free, and keeping it there. Increase slowly as you tolerate. That said, first confirm you’re not allergic, intolerant or sensitive to any of the ingredients! ~DrKF
I know this is an older post, but my nutritionist suggested that I try SBI protect and you mention that people with chronic constipation need to go slower and work up to the recommended does. Is there anything you can do to keep the bowels moving while taking SBI Protect? Thank you.
There are tons of complementary methods to ensure continued “flow”. Speaking generally, supplements like magnesium citrate, triphala, certain fibers, probiotics, as well lifestyle practices that support motility like diaphragmatic breathing and gargling (just to name a few). Work with your nutritionist to identify the best options that fit into your plan.